Soft lenses that correct keratoconus have been available for around 13 years in hydrogel form. Although they work well, there has always been concern about possible vascularisation (as with Hybrid lenses) if lenses are worn for long periods of time. With the advent of lathe cut silicone hydrogel materials, these lens types now allow up to even 18 hours comfortable, healthy wear. This is extremely important to keratoconics, as they are reliant on their lenses for functional vision.
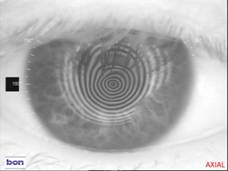
Many question how a soft lens can correct anything other than mild to moderate keratoconus – surely the lens simply reproduces the corneal irregularity? Rigid gas permeable (RGP) lenses work by providing a smooth rigid front optical surface – but the fit has to be just right – too flat and the lens will abrade the cornea, too steep and the resultant tear film below the lens will reduce acuity through induced higher order aberrations. (Fig 1)
Silicone hydrogel soft lenses have just enough flexibility to take up the corneal shape on the back surface but enough rigidity to produce a smooth front optical surface (Fig2)
 |
 |
| Fig 1 |
Fig 2 |
One perceived difficulty in refitting RGP wearers, especially keratoconics, into soft lenses is the “de-moulding” effect as the cornea recovers from the compression imparted by the RGP lenses. However, many patients do well with a straight transfer over from one lens type to the other.
Case 1
MC is a 40-year-old male who had been wearing Rose K RGP lenses for keratoconus for 20 years. He had never achieved more than 6/36 in the RE and was reliant on the vision from the LE for driving. At a recent hospital appointment, he was told that his acuity had now dropped below driving standards and, as no other contact lenses could be found to improve vision, he was offered bilateral grafts despite the corneas being clear. As there is a waiting list for NHS grafts, he was told the procedures for both eyes would take a total of 6 years to complete.
Initial examination
The right cornea demonstrated advanced and the left moderate keratoconus and both showed mild central haze but no definite scarring. The fit of both RGP lenses was quite flat and in order to prevent the lenses from “popping out”, he tended to move his head rather than his eyes.
| RGP lens acuity: |
R: 6.10/8.70/-10.75 VA 6/36 |
L: 7.10/8.70/-11.50 VA6/18 |
| Sim Ks: |
R: 5.70 x 31/4.92 x 121 |
L: 6.38 x 100/5.46 x 262 |
He was fitted with silicone hydrogel lenses for keratoconus [Silicone Hydrogel - 74% water content, modulus 0.38, Dk 60 (as stated on UltraVision and Contamac websites)]
R: 8.20/14.50/-14.50/-4.00 x 45 VA 6/12 + L: 8.20/14.50/-14.00 DS VA 6/7.5
He was warned of possible refractive changes as the corneas “de-moulded” from the compression caused by the RGP lenses, but although he noticed changes, especially in the first 2 weeks, at all times acuity was better than his previous RGP lenses.
3-month follow up:
Slit lamp: Corneas were now clearer and the topography and keratometry showed a much improved corneal surface quality. Visual acuity in the lenses had improved in both eyes to R: 6/9 and L: 6/6 with no over refraction necessary.
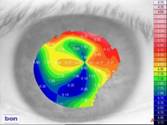
| RE Corneal keratometry at initial visit |
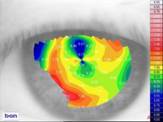
RE Corneal keratometry at 3-month visit |
|

|
Fig 3 shows improvement in corneal shape over 3 months |
 |
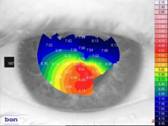 |
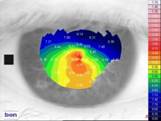
| RE topography at initial fit |
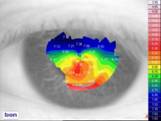
RE topo after 3 months |
 |
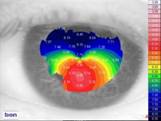 |
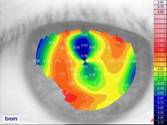
| LE topography at initial fit |
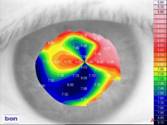
LE topo after 3 months |
Discussion
Although MC had reported some fluctuation of vision over the 3-month period, at no time was his vision as poor as it had been in the RGP lenses. Topography shows how the corneal shape has normalised after converting to silicone hydrogel wear. The “before and after” RE placedo rings in particular show a marked improvement in regularity after converting to silicone hydrogel wear.
He reported much increased comfort and reduced photophobia and is delighted his vision is the best it has been for 20 years. He is no longer being considered for grafting.
Case 2
GB is a 39-year-old male who had been grafted 20 years previously because he could not be fitted with suitable contact lenses – even though he had clear corneas. He managed with just spectacles for many years but eventually, keratoconus reasserted itself in the right graft and he had to resume contact lens wear.
He presented wearing RGPs and achieving 10 hours wear with 6/5 acuity R & L.
| Spectacle Refraction: |
| R +1.00/-7.50 x 105 VA 6/7.5 |
L +3.00/-4.00 x 100 VA 6/7.5 (full correction not tolerated) |
| RGP lenses: |
| R:7.40/7.90:7.00/8.00/8.50:9.00/12.25:9.40/+0.75/-5.50 VA 6/5 |
L: Rose K 8.00/10.40/-1.00 STD edge lift VA 6/5 |
Silicone hydrogel contact lenses for keratoconus were fitted [Silicone Hydrogel - 74% water content, modulus 0.38, Dk 60 (as stated on UltraVision and Contamac websites)]:
R:8.60/14.50/+1.25/-6.50 x 98 VA 6/5 L: 8.60/14.50/+1.00/-2.00 x 90 VA 6/5
He initially asked to be fitted in soft lenses only so that he could compete in motor rallies, as the competition rules disallowed RGP lenses. However, as the acuity equalled that of his RGPs and he achieved 18 hours uninterrupted wear in the lenses, he opted to convert totally to silicone hydrogel lenses.
At the 3-month follow up, the lenses were changed to:
R:8.60/14.50/+1.25/-8.50 x 102 VA 6/5 L: 8.60/14.50/+2.50/-3.50 x 103 VA 6/5
Lenses were changed at 6 months and remained the same at 9 months follow up:
R:8.60/14.50/+0.50/-8.50 x 102 VA 6/5 L: 8.60/14.50/+2.50/-3.50 x 103 VA 6/5
 |
 |
| RE topography at initial fit |
RE after 6 months |
 |
 |
| LE topography at initial fit |
LE after 6 month |
Discussion
The RE fluctuated most during the settling down period and, at around 5 months, VA dropped to 6/12+ for around 2 weeks then started to improve again. Apart from that short period, GB did not experience any visual discomfort from his silicone hydrogel lenses.
What is significant about this case is that the patient himself considered he was a success story with RGP lenses. It was not until he converted to SiH that he realised that the significant photophobia from which he suffered was a result of RGP wear, not the condition itself. Previously he had to wear wrap round sunglasses with an extremely dark tint all the time outdoors, whatever the weather, and for much of the time indoors. Now he wears sunglasses much like any person with normal corneas would and attains exactly the same acuity (6/5) that he did with his RGP lenses. Many feel that only RGP lenses can give good vision with irregular corneas but in fact excellent acuity is possible with silicone hydrogel lenses.
The difference in wear time was very important to him: “When wearing RGPs I had to choose when to see because 10 hours wear in RGPs meant no vision after work. To maintain 10 hours wear at work, I had to leave them out at the weekend. I simply did not see my children grow up – silicone hydrogel lenses gave me my family life back.”
|



