Everyday I am grateful for the advances in contact lens technology such as silicone hydrogel designs, which have enabled me to successfully fit more patients with contact lenses. Beside the significant benefit of the high Dk/t removing the risk of hypoxia to the cornea, silicone hydrogels also offer greater biocompatibility for lens wearers who work long hours in low humidity air conditioning, presumably due to the lower water content dependent and more lubricating surface properties of the polymers. A large percentage of my borderline dry eye patients who struggled to maintain a comfortable and useful daily wear time with their soft lenses are happy converts to silicone hydrogels. Given that around 40% of lens wearers complain of dry eye symptoms (Doughty et al 1997), silicone hydrogels are a logical first choice for all my new two week and one month lens fits too. However, I have learned that success is not assured simply by fitting a silicone hydrogel lens and re-issuing the patient’s customary care solution.
In my practice, fitting silicone hydrogels has been complicated by an estimated 20% adverse response rate often resulting in unexpected discomfort and dryness and in some cases, heavy surface deposits, CLPC, conjunctival inflammation and corneal staining.
The factors influencing successful silicone hydrogel lens wear are complex. There are patient specific factors such as tear chemistry, tear volume, matching limbal topography to the edge fit of the chosen lens design, sensitivities to disinfecting agents, and lens care compliance (e.g. rubbing versus no rubbing). Then there are silicone hydrogel lens specific variables for each design, such as edge thickness profile, modulus of elasticity, lubricity, wettability and deposit resistance of the surface, the integrity of any surface treatment on the lens and very importantly I have come to observe - the degree of chemical interaction of the surface polymer and bound lipo-protein deposits with compounds such as buffers and biocides from disinfecting solutions and lubricants.
Practitioner related factors such as design selection, technical fitting skill, recognition of early inflammation of the cornea and conjunctiva and awareness of the respective chemical formulations of disinfecting solutions also play a pivotal role in fitting success. Ensuring smooth optimal fit of the silicone hydrogel edge to the limbal conjunctiva is critical for patient comfort and demands more fitting skill from the practitioner than with older more flexible lens materials where a “one base curve fits all” approach will work more often. Lens edge lift off which irritates the tarsal plate is less likely with the recently released lower modulus generation of silicone hydrogel polymers such as O2Optix, Oasys and Biofinity than stiffer first generation materials of Focus Night&Day and Purevision.
So assuming the chosen lens design has been correctly fitted, that the tear volume is sufficient and there is no CLPC, why do some wearers develop hypersensitivity responses and discomfort even within hours of using a daily wear silicone hydrogel lens? Are wearers sensitive to the polymer material or to the effects of the disinfecting agents?
 |
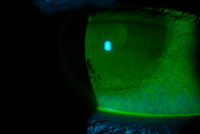 |
Figure 1 - click to enlarge |
Figure 2 - click to enlarge |
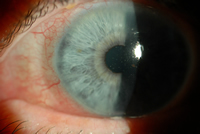
One of my cases (GM), a -2.00 D myope, had successfully worn Proclear multifocal lenses in combination with Complete disinfecting solution. After complaints of mild dryness, I refitted him with a Purevision multifocal lenses and he continued with his customary Complete solution. By one week, he discontinued lens wear due to dryness after 4 hours accompanied by poor vision and increased mucous secretion and redness (Figure 1). There were mild tarsal plate changes, corneal SPK and conjunctival staining (Figure 2). New Purevison lenses were dispensed with a change to Optifree disinfecting solution and the symptoms did not return.
After some months (GM) then swapped to using Aquify (recommended for silicone hydrogels) and he again became symptomatic after one week. This outcome suggests that the Complete chemical formulation somehow interacted with the Purevision Balafilcon anterior lens surface to increase deposition and reduce wettability in a way that did not occur with the Proclear lens surface for this patient. The adverse response indicated an incompatibility of Balafilcon material with Complete for this patient. Aquify shares the same disinfectant base as Complete, polyhexamethylene biguanide (PHMB) which may account for the similar result when used by this patient. PHMB (in the form of ReNu disinfecting solution) has been previously implicated in the disruption of epithelium i.e. staining, when used in combination with Purevision Balafilcon (Jones et al 2002, Andrasko et al 2006) and Focus N&D (Dumbleton et al 2006).
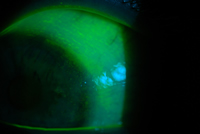
In the case of patient GM, what role did the disinfection solution have in creating heavy surface deposition and staining? Did the solution interact/bind with the Balafilcon material in a way which served to irritate the eye and increase levels of lipid, mucin and presumably some protein deposition? As the patient could successfully use Complete with a non-silicone hydrogel lens I can only speculate that it did. Patient GM can also successfully wear Purevision lenses in combination with Optifree indicating that he has no sensitivity to Balafilcon material itself. With regard to staining, hydrogel lenses have also been shown to absorb and release disinfecting/soaking solution biocides from the lens matrix into the eye during wear. The rate and concentration of biocide release varies between disinfecting solutions and materials and is implicated in corneal damage as disclosed by fluorescein staining (Andrasko et al 2006, Papas et al 2006). This was demonstrated by Patient MH who used Aquify and was asymptomatic with minimal surface deposits after one week but showed differential cytotoxic staining with different silicone hydrogels. The eye wearing Acuvue Oasys showed mild redness, significant limbal and corneal staining compared to the eye wearing Acuvue Advance (Figures 3 and 4). Repeating the lens trial with new lenses and AOSept replacing Aquify resulted in no staining for either eye, again suggesting the sensitivity is with the solution formulation and not the silicone hydrogel materials.
 |
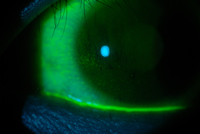 |
Figure 3 - click to enlarge |
Figure 4 - click to enlarge |
Recently several patients successfully using Optifree with their silicone hydrogel lenses (O2Optix and Acuvue Oasys) developed intolerance to lens wear within weeks of swapping to the new Optifree Replenish solution yet the majority of users seemingly continue successfully. The interaction of the lens material with the differing solution components and a specific patient tear chemistry/ immune response again appear to be the likely explanations for who develops cytotoxicity responses and who does not.
In my experience, disinfecting solutions containing PHMB, which comprises the majority of multipurpose solutions on the market, are more likely to create an ocular hypersensitivity response in a silicone hydrogel wearer than a Polyquad based solution, but currently choosing the optimal multi-purpose solution for any new silicone hydrogel fit is still guesswork. The increase in rate of hypersensitivity response emphasizes the need for diligent patient aftercare and further research to address silicone hydrogel material /solution incompatibilities.
It would be extremely useful clinically if I could predict who will be sensitive to the use of specific solutions with a given silicone hydrogel material before I dispense. Perhaps silicone hydrogel lens manufacturers could research their lens polymer performance using the range of more popular disinfecting solutions and advise us of the most compatible solution with their material. Ideally a more biocompatible multi-purpose disinfecting solution for silicone hydrogels will soon be available. Meanwhile hydrogen peroxide based disinfection may be less user friendly but it is associated with least ocular hypersensitivity response (Carnt NA et al 2007), provided it is used according to instructions. In order to gain maximum clinical benefit from fitting the range of silicone hydrogel materials now on offer and to avoid the risk of hypersensitivity responses associated with currently available multi-purpose solutions, hydrogen peroxide may need to become my preferred disinfection regimen.
References:
- Doughty MJ, Fonn D, Richter D, Simpson T, Caffery B, Gordon K, A patient questionnaire approach to estimating the prevalence of dry eye symptoms in patients presenting to optometric practices across Canada. Optom Vis Sci 1997;74:624-31
- Jones L. MacDougall N, Sorbara LG. Asymptomatic corneal staining associated with the use of Balafilcon silicone-hydrogel contact lenses disinfected with polyaminopropyl biguanide-preserved care regimen Optom Vis Sci 2002;79:753-61
- Dumbleton K, Keir N, Moezzi A,Feng Y, Jones L, Fonn D. Objective and
subjective responses in patients refitted to daily wear silicone hydrogel contact lenses. Optom Vis Sci 2006;83:758-68
- Adrasko GL, Ryan KA, Garafolo RJ et al. Compatibility of silicone hydrogel lenses with multi-purpose solutions. Invest Ophthalmol Vis Sci 2006;47:E-abstract 2392
- Papas EN, Naduvilath T, Jalbert I. Inflammatory consequences of care product induced (toxic) corneal staining during soft contact lens daily wear. Paper presented. BCLA. Birmingham UK, 2006.
- Carnt NA, Jalbert I, Stretton S et al Solution toxicity in soft contact lens daily wear is associated with corneal inflammation. Optom Vis Sci 2007;84:309-15
|



 Narelle Hine, MSc(Optom), Dip App Sc (Optom), DCLP, FAAO
Narelle Hine, MSc(Optom), Dip App Sc (Optom), DCLP, FAAO