|
Changes
It is widely accepted that contact lens wear can lead to changes in corneal curvature and the impact of these changes on the corneal epithelium has only recently become clear. These effects may be responsible for the post operative refractive changes in patients who have undergone laser refractive surgery. (1,2) Prior to the pre-operative examination, contact lens wearers frequently need to discontinue wear for weeks, so that the cornea can to return to its baseline shape. A refractive surgery centre in the Netherlands reported that 95% of all re-treatments for refractive reasons were performed on previous contact lens wearers. (3) Currently, cessation of rigid gas permeable (RGP) lens wear is advised for at least eight weeks prior to laser surgery. After this, the cornea needs to be evaluated at two-week intervals until a stable topography is reached. Stable topography is usually defined as a change of 0.50D or less, compared to the last visit.
Both RGP and soft contact lenses can alter corneal topography. A recent report by Muriel Schornack (4) estimated that 27% of all cases of corneal warpage are found in patients wearing hydrogel lenses. These topographical changes are thought to be primarily the result of hypoxia, and indeed are more commonly seen in patients wearing conventional hydrogel lenses. The cause of this could be the lens thickness and low Dk materials. For example, topographical changes are regularly seen in prism ballasted toric hydrogels which are made out of conventional materials. Due to the potential for changes in corneal curvature with soft lens wear, at least two weeks of discontinuation of these lenses is advised prior to pre-operative examination, followed by two week interval checkups to assess the corneal stability, before laser surgery can be considered.
Challenges: Case study
A 49 year old female hydrogel lens wearer was referred to an ophthalmologist due to an unexplained decrease in the visual acuity of her left eye. The patient wore spherical monthly replacement lenses, made from conventional hydrogel material. Refraction without lenses did not improve her vision. Her refractive error and optimal acuity is shown below.
Refractive error OS: -4.75/ -1.75 x 40 VA 0.4 (logMAR units)
Slit-lamp examination revealed an unremarkable cornea. Further investigation using topography was then conducted. Figure 1 shows the OS corneal topographical map shortly after lens removal.
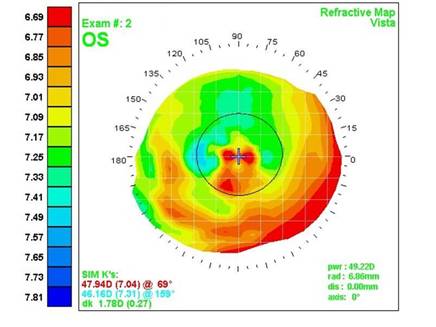 |
| Figure 1: Corneal topography shortly after hydrogel lens removal. (Courtesy of Marco van Beusekom, Visser Contactlenzen, the Netherlands) |
The irregularities in the centre of the map displayed in Figure 1 offers an explanation as to the cause of the reduction in the patient’s visual acuity.
After lens removal, the cornea returned to normal. Figure 2 displays a symmetrical topographical map with limited central corneal astigmatism The patient’s visual acuity had returned to 1.0 (logMAR), although unfortunately she dropped out of contact lens wear after this incident.
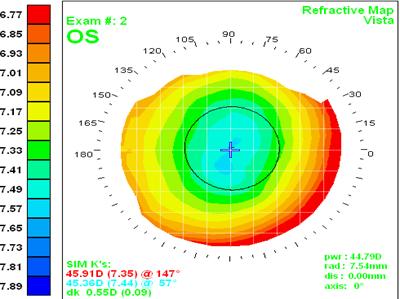 |
| Figure 2: Repeated corneal topography after hydrogel lens removal. (Courtesy of Marco van Beusekom, Visser Contactlenzen, the Netherlands) |
Although some changes to the corneal topography caused by hydrogel lens wear can be detected during a slit lamp assessment – as demonstrated in Figure 3, these findings are very rare.
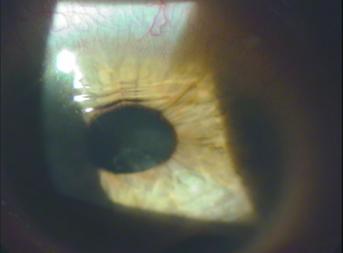 |
| Figure 3: An unusual case of severe peripheral corneal disruption underneath a conventional toric hydrogel lens, which is even visible to the human eye with a slitlamp. (Courtesy of Hans Kloes, Kloes Eye Kliniek, the Netherlands) |
The topographical changes under a hydrogel lens are usually subtle and should be monitored on a routine basis. Distortion of keratometry mires can be a first indication, but this measurement is limited to a small (usually 3mm) central portion of the cornea, and the changes observed can not be easily classified. Corneal topography however covers a large, if not the total, area of the cornea and the application of softwear to create difference maps between visits can identify subtle topographical changes promptly and accurately.
The arrival of silicone hydrogel contact lens materials has led to a reduction in the hypoxia related corneal warpage cases observed with soft lens wear. However, the early versions of silicone hydrogel lenses caused a different type of distortion due to the higher modulus of the material compared to conventional hydrogels. This was especially evident in the peripheral cornea, where changes were not uncommon. Despite the improvements in these lenses (in particular the newer generation silicone hydrogel lenses that have a lower lens modulus), practitioners should still maintain their awareness of the potential for topographical changes.
Chances
Interestingly, topographical changes to the cornea can also be used to the advantage of the lens wearer.
Studies at the University of New South Wales (5) showed significant corneal flattening (0.61 +/- 0.35D p=0.014) within ten minutes of orthokeratology lens wear. Orthokeratology lens wearers around the world now benefit from the temporary topographical changes that specially designed RGP lenses create.
There have been some anecdotal reports of orthokeratology-like changes with silicone hydrogel lenses. Patients who accidentally wore silicone hydrogel lenses inside out have reported improvements in their vision upon removal of the lenses, and subsequent examinations have indicated decreases in myopic refractive error. This phenomenon was first described by Patrick Caroline at the British Contact Lens Association Meeting in June of 2003. Practitioners should be aware of this effect, since no apparent decrease in lens wearing comfort is usually noted when the silicone hydrogel lenses are worn inside-out. The effect is found to be more pronounced in silicone hydrogel lens wearers who have a higher degree of myopia. The topographical effect is similar to a (successful) orthokeratology lens fit with RGP lenses. Figure 4 displays the topography map of a patient who wore a CIBA Focus Night & Day lens (base curve 8.4, -10.00D diameter 13.8 mm) inside-out (deliberately) on a continuous wear basis for 30 days. A 3.12D reduction in myopia in the centre of the topography is noted.
 |
| Figure 4: Topography map demonstrating the corneal curvature before inverted silicone hydrogel lens wear (TOP LEFT), one month after lens wear (BOTTOM LEFT) and the difference map determined between them (RIGHT) (Courtesy Patrick Caroline, Pacific University, Oregon USA) |
Research is underway to investigate whether these lenses can be used to purposely change the shape of the cornea in order to temporarily reduce myopia. Pilot studies at the Pacific University College of Optometry demonstrated that significant topographical changes can be induced by the overnight wearing of inverted, minus powered, silicone hydrogel lenses. They also found that patient comfort was not affected by lens inversion.
It is clear that further work needs to be done to better understand the nature and extent of the corneal changes associated with the accidental wearing of inverted silicone hydrogel lenses. However, the preliminary findings indicate that in the future, it may be possible for silicone hydrogel materials to be used to temporarily alter the shape of the cornea and therefore the magnitude of the refraction, in a controlled way.
In summary
The topography of the cornea in all types of lens wearers should be monitored closely. Low Dk, thicker conventional hydrogel lenses e.g. toric designs, should be avoided as far as possible, and replaced with silicone hydrogel lenses.
Despite the reduction in hypoxia related topographical changes with the increased use of silicone hydrogel lenses, mechanical changes (due to the high modulus) still can be seen. These have however been partly overcome with the use of the newer generation silicone hydrogel lenses that have a lower lens modulus.
On the positive side: future controlled alteration of the corneal shape at night with silicone hydrogel lenses could be useful in the temporarily correction of small amounts of ametropia.
- Wang X, McCulley JP, Bowman RW, Cavanagh HD. Time to resolution of contact lens-induced corneal warpage prior to refractive surgery. Clao J 2002;28:169-71.
- Budak K, Hamed AM, Friedman NJ, Koch DD. Preoperative screening of contact lens wearers before refractive surgery. J Cataract Refract Surg 1999;25:1080-6.
- Lafeber R. Personal communication. 2004.
- Schornack M. Hydrogel contact lens-induced corneal warpage. Cont Lens Anterior Eye 2003;26:153-9.
- Sridharan R, Swarbrick H. Corneal response to short-term orthokeratology lens wear. Optom Vis Sci 2003;80:200-6.
|



