Case Study 1
KW, an 11 year-old female, first reported to the Cornea and Contact Lens Clinical Service in a multidisciplinary health care setting on October 12, 2005. She was wearing spectacles at the time of her examination. Her chief complaint was distance blur with her habitual spectacle correction. She enjoyed school, swimming, dancing, and cheerleading. Her systemic history was remarkable for sickle cell anemia. Family health history was non-contributory to the contact lens examination. She had been examined periodically in the College clinic since 2002, having her most recent eye health and vision examination one month preceding the contact lens appointment. Having previously discussed contact lenses with her parents and the referring doctor, she presented to the Clinical Service with the anticipation of being fit with contact lenses.
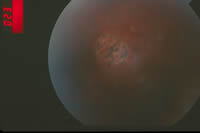
Her examination revealed a modest increase in refractive error. Manifest refraction revealed simple myopia (OD -1.75 DS 20/20 and OS -1.75 DS 20/20). Ocular health evaluation revealed a healthy anterior segment. Her recent dilated fundus examination revealed intact retinal vasculature, clear maculae, and non-proliferative sickle cell retinopathy (sunbursts, salmon patches, and fibrosis). Binocularity was within normal limits.
|
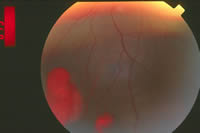 |
| Figure 1a and 1b. Non-proliferative sickle cell retinopathy |
click to enlarge |
Table 1. Contact lens parameters 2005 |
| Eye |
Lens type |
Base curve radius (BCR) |
Overall Diameter (OAD) |
Power |
OD |
galyfilcon A |
8.7 mm |
14.0 mm |
-1.75 D |
OS |
galyfilcon A |
8.7 mm |
14.0 mm |
-1.75 D |
Table 2. Contact lens parameters 2006 |
Eye |
Lens type |
Base curve radius (BCR) |
Overall Diameter (OAD) |
Power |
OD |
lotrafilcon B |
8.6 mm |
14.2 mm |
-2.25 D |
OS |
lotrafilcon B |
8.6 mm |
14.2 mm |
-2.25 D |
Contact lenses were dispensed with the parameters above (Table 1). A daily wear schedule with two week replacement was prescribed. Proper lens care and handling was reviewed with the patient prior to dispensing. She reported for follow-up care on November 3, 2005 and on November 22, 2005. Although she missed her subsequent contact lens follow-up visit, she returned for a comprehensive examination on September 28, 2006. Diagnostic lenses were dispensed with a modest change in prescription. The brand of silicone hydrogel lens material was changed based upon the preferences of the prescribing doctor, rather than in response to a presenting problem (Table 2).
In summary, her initial contact lens experience was trouble-free. She reported excellent vision and comfort. At the age of 12, she has enjoyed almost one year of successful contact lens wear, without incident.
Case Study 2
At the age of 11, AW is also a veteran contact lens wearer. Like KW, she enjoys good health and excellent vision. She has a slightly higher refractive error (OD -3.00 DS 20/20 and OS -2.75 DS 20/20) and began wearing her vision prescription full time around the age of ten. She has worn contact lenses for approximately two years, initially only for dance class and special occasions and, more recently, during school. While she initially experienced some difficulty with lens insertion, she has consistently reported clear vision and excellent comfort. She is compliant with her follow-up care. Over recent months, she has eschewed her pink spectacle frames and Barbie case in exchange for dark purple frames and a black case. She now appears to be as interested in the cosmetic benefits of contact lenses as in the functional ones.
Discussion
Unlike Case Study 1 where I viewed this patient’s care from the perspective of an eye care provider, in Case Study 2 my perspective was that of a parent. Now that I have a view from “both sides” I have become increasingly receptive to fitting cosmetic contact lenses in preteens, although I continue to follow the parents’ or guardians’ lead before presenting contact lens options. In Case Study 2, I initiated the contact lens fitting, suggesting to my daughter that she might enjoy “being the first” [in her class] to wear contact lenses. This discussion followed a previous conversation where she lamented that she was “never first” among her peers with any milestones, with the most recent comparisons being made regarding cell phone use.
Caring for this age group requires patience. Tweens wish to blend in. When confronted with a situation where they stand out, tweens can become emotional. Additionally, tweens may be very sensitive to situations where they believe they are being treated like a young child. While the parents or caregivers may believe that the child is “too young for that,” the tween believes that he or she is “too old for that.” Despite this cynicism and self-perceived maturity, a tween may exhibit the exuberance and awe of a child when experiencing contact lens-corrected vision for the first time.
Beyond the psycho-social factors characteristic of this generation of lens wearers, the actual contact lens fitting and aftercare for the tween is generally straight-forward. The value of silicone-based lens materials in managing refractive error in children has been recognized since the introduction of the Silsoft lens by Bausch and Lomb (Rochester, New York) for pediatric aphakia. Silicone’s high oxygen permeability is advantageous for young patients with a lifetime of contact lens wear ahead of them. Tweens generally don’t complain about the contact lens associated discomfort that can be the bane of older lens wearers. Lens materials continue to improve so this generation has much to look forward to.
While business analysts have been quick to recognize their economic power, tweens’ influence is based upon the financial resources of parents and other adults. So, although the tweens’ influence is real, parents are influential in health care decisions where they recognize a potential risk to the child’s well being. Therefore, the eye care practitioner should be cognizant of both adult and tween expectations when caring for this demographic group. While parents of this generation generally embrace contact lens wear as routine, and recognize it as a rite of passage into adolescence or adulthood, they are looking for a safe and trouble-free lens wearing experience. As in many things in life, team work breeds success and in this instance, a life-time of happy and healthy contact lens wear.
References
- Sankaridurg P.Contact lenses for tweens. (2004) Available from http://www.siliconehydrogels.com/editorials/previous_editorial_padmaja.asp
Accessed September 30, 2006.
- Wikipedia Encylopedia. Tween. (2006) Available from http://en.wikipedia.org/wiki/Tween. Accessed September 30, 2006.
Acknowledgements: Photograph submitted by Marc B. Taub, OD, FAAO |