| Introduction BP is a 65 year old white female who had undergone hexagonal keratotomy for the correction of hyperopia 12 years prior. She reported considerable difficulty with visual performance postoperatively and could only be managed with spectacles of unknown correction. Three years prior to her office visit, she had undergone bilateral cataract extractions with phacoemulsification and continued with spectacle correction. She presented to determine whether she was a suitable candidate for LASIK.
Case Study Uncorrected visual acuity (UCVA) was 20 / 80 OD with 20 / 40 OS at distance when viewing an EDTRS chart and 20 / 40 OD with 20 / 125 OS at near with a ETDRS near point card. With a refraction of -1.75 +0.25 X 111 OD and -1.00 +1.00 X 140 OS, best spectacle corrected visual acuity (BSCVA) was 20 / 25 in both eyes. Intraocular pressures for both eyes were 17 mm Hg.
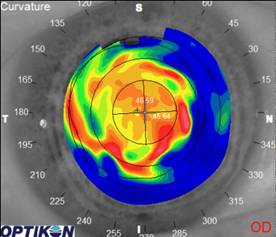
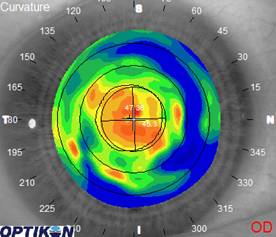
Corneal curvature was measured using manual keratometry and were 45.50 @ 161 combined with 47.00 @ 071 OD, and 46.50 @ 058 combined with 46.75 @ 148 OS. The balance of her dilated eye examination was unremarkable internally. External ocular evaluation revealed significant scarring and disorganization centrally with the apparent hexagonal scars radiating outwards.
Corneal topography revealed considerable irregular astigmatism with disorganized optical zones, see Figure 1.
 |
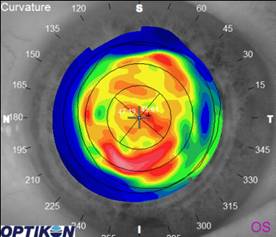 |
Figure 1 |
A pair of high Dk silicone hydrogel lenses were fit using 8.4 mm base curves and +.50 OD with -0.50 OS. These powers were chosen in an attempt to maintain the patient’s monovision status, whilst improving her visual quality and performance. With the lenses in place, best corrected low contrast visual acuity (BCLCVA) was 20 / 70 OD with 20 / 25 OS at distance, and 20 / 15 OD with 20 / 60 OS at near. The patient reported excellent comfort.
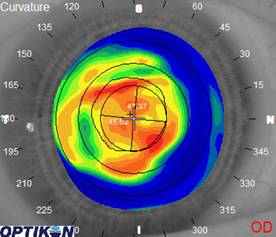
Corneal topography revealed some slight improvement in the level of disorganization of the optical zones, see Figure 2. From the patient’s perspective, her vision was considerably better.
 |
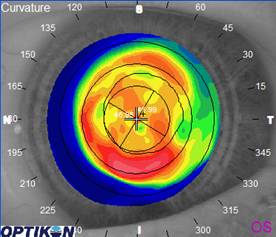 |
Figure 2 |
Follow-up visits At the 2-week follow-up visit, the patient reported excellent comfort and noted that she no longer felt dizzy, a complaint which had not been deduced from prior visits.
BCLCVA was 20 / 40 OD with 20 / 32 OS at distance, and 20 / 25 OD with 20 / 100 OS at near. Over-refraction of the lenses suggested the need to change powers to -0.50 OD and +1.00 OS using the same silicone hydrogel in the 8.4 mm base curve.
After removal of her contact lenses, measured refractions were -1.50 +1.00 X 073 OD and -0.25 +0.75 X 142 OS yielding 20 / 25 and 20 / 20 BSCVA. The patient was advised to continue wearing the lenses, but only in daily wear format. She was instructed on the use of peroxide-based solutions for disinfection and cleaning. Follow-up visits at 2 months and 6 months were unremarkable.
One year after contact lens wear, the patient is doing well. She can wear her lenses approximately 10 to 12 hours per day without incident. At the one year follow-up visit, BCLCVA was 20 / 60 OD with 20 / 32 OS at distance, and 20 / 40 OD with 20 / 100 OS at near. Over-refraction was -0.75 +0.50 X 082 OD yielding 20 / 20.
Corneal curvatures measured by manual keratometry were 44.75 @ 173 combined with 46.25 @ 083 OD and 46.00 @ 031 combined with 46.75 @ 121 OS. The optic zone areas were considerably better organized (Figure 3) with noted improvement in visual quality by the patient. She was prescribed the same 8.4 mm silicone hydrogels with plano OD and +1.00 OS to be worn daily and asked to return for follow-up in 6 months time.
 |
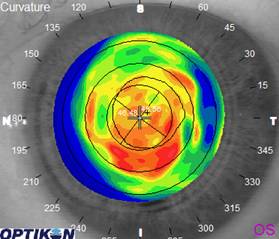 |
Figure 3 |
Discussion Irregular astigmatism is a noted clinical finding with hexagonal keratotomy which ultimately contributed to the demise of this surgical procedure. Irregular astigmatism was certainly the outcome for this patient as well. Her optical zones were disorganized resulting in diminished visual performance.
The improvement in visual quality and performance for this patient after wearing silicone hydrogels is interesting. It is possible that the slightly ‘stiff’ lens material may have contributed to the redistribution of corneal tissue and a better optical outcome, or that performance was improved through a bandage-like effect brought on by the overlying contact lens.
The use of silicone hydrogel lenses for this patient was definitely beneficial. Although it cannot be assumed that all patients with irregular astigmatism will benefit from the application of silicone hydrogels, practitioners should remain open to the advantages that these lenses can provide for patients with difficult eyes. |



 Gregg Eric Russell, OD, FAAO
Gregg Eric Russell, OD, FAAO