| Case 1:
CR is a 42 year male solicitor who had worn RGP contact lenses
for 20 years. He reported no medical problems or allergies and
no previous surgery. CR presented for the first time to the practice
complaining of reduced wearing time and contact lens intolerance.
He was finding it particularly difficult to manage a full working
day in front of a VDU screen in an office environment.
| Spectacle Rx: |
Keratometry readings:
|
RGP lenses: |
| R-8.50/-0.50x90 6/5 |
R 7.77mm (43.25D)/ 7.70mm (43.62D) |
HDK 701 |
| L-9.50/-0.50x90 6/5 |
L 7.88mm (42.62D) / 7.80mm (43.12D) |
R 7.80:9.30 -7.25 Over Rx Plano 6/5 |
| No reading addition |
|
L 7.80:9.30 -7.75 Over Rx -0.50 6/5 |
| |
Add +1.00 for near comfort |
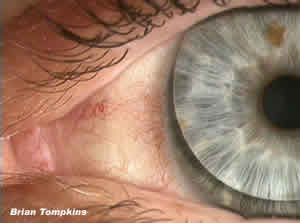 |
| Figure 1: Bulbar and limbal
conjunctival injection with previous RGP in situ. |
Slit Lamp examination showed marked 3 & 9 o'clock staining
at an 11.00 a.m. appointment, graded as at least 2.50 on the Efron
scale(ES), with a similar grade of conjunctival injection within
the palpebral aperture (Figure 1).
High magnification examination of the corneal area adjacent to
the limbus showed neovascularisation and engorged vessels associated
with the exposed and compromised cornea (Figure 2). CR was also
found to have a grade 1.5 meibomian gland dysfunction for which
he started immediate treatment with "Lid Care" and heat
and massage.
CR was initially trial fitted with a pair of Focus N&D 8.40
-8.00DS (slightly over corrected). He was instructed in handling
and lens care (Focus Plus) and after settling and refraction was
dispensed with -7.50 R&L. This gave a slightly under corrected
LE which he enjoyed for monovision for his office work. Initial
wearing schedule was advised at 1 week of DW and then review.
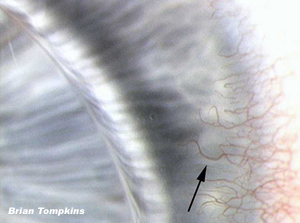 |
| Figure 2: High magnification
of neovascularisation and limbal hyperemia with previous RGP
in situ. Arrow indicates reference vessel. |
Best CL Rx was then found to be:
R -7.25 6/5
L -7.50 6/6-2, Over Rx -0.50 6/5 Ready Readers of +1.00 gave
N5 which were dispensed from stock and the patient was instructed
to return at 9.15am after his 1st overnight.
The 1st overnight follow-up showed no problems. Conjunctival
injection was down to approximately 1.00 ES, but symptoms of intermittent
blurring led me to advise artificial tears as examination showed
some lipid contamination. He was also instructed to continue with
EW until the next appointment , but to remove the lenses to rub
and rinse if they felt smeary.
At the end of the first month the neovascularisation had reduced
to ghost vessels and the conjunctival injection was also significantly
reduced (Figure 3). The lipid problem remained and he is now on
a pattern of flexible wear to suit his schedule. He continues
with "Lid Care" and artificial tears as needed. The
wearing time is now generally all waking hours with occasional
EW as required.
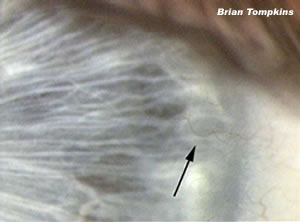 |
| Figure 3: High magnification
of ghost vessels and reduced limbal hyperemia following 1
month of EW with Focus N&D lenses. Arrow indicates reference
vessel from Figure 2. |
All images taken with Eyecapture. |


