CH, a 39-year old Caucasian female, presented for an unscheduled visit with complaints of periodic episodes of sharp eye pain OS>OD that lasted a few minutes over the previous few weeks. She was a rigid gas permeable contact lens wearer for moderate myopia for over 15 years without complications. She had been seen for a comprehensive eye examination 3 months prior, when epithelial basement membrane dystrophy (EBMD) OS>OD were diagnosed. Her ocular and medical histories were otherwise unremarkable.
Entering visual acuities with spectacles were OD 20/20 and OS
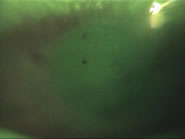
20/20-. Biomicroscopy revealed geographic areas of positive and
negative fluorescein staining and basement membrane irregularities
of both corneas (Figure 1, 2, 3). Lids, conjunctiva, anterior
chambers, and crystalline lenses were clear and quiet OU.
 |
 |
 |
| Figure 1: The right eye of the patient,
showing two small areas of negative staining in the superior
cornea,
indicating
areas
of EBMD - click to enlarge |
Figure 2: The left eye of the patient,
showing a larger
> map-like area of negative staining in the nasal mid-peripheral cornea - click
to enlarge |
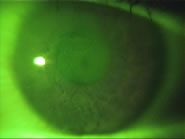
Figure 3: A close-up of image 2 - click
to enlarge |
The patient was diagnosed with epithelial basement membrane dystrophy with mild epithelial erosions OU. GP lens wear was discontinued. She was placed on Celluvisc lubricants tid and instructed to return for a follow-up in 1 month. At the 1 month visit, she noted that she continued to have occasional flare-ups, which resulted in mild discomfort OU. To more effectively manage her recurrent epithelial erosions, she was refit her into soft contact lenses to provide a bandage effect and decrease mechanical interaction caused by her GP lenses. She was refit into Bausch & Lomb PureVision silicone hydrogel contact lenses with parameters of OD 8.6 / 14.0 / -3.50 and OS 8.6 / 14.0 / -4.00. These lenses were selected to both bandage the cornea and provide sufficient oxygen to prevent corneal edema. She was put on a daily wear schedule, and averaged 8 hours of lens wear per day. She reported good vision and comfort, and at each of her 6 month follow-up visits and comprehensive exams over the following two years, reported no additional episodes of sharp pain or discomfort.
The following year, CH returned for her annual comprehensive eye exam. At this visit, because PureVision was no longer available, CH was refit into Ciba Focus Night & Day silicone hydrogel contact lenses with parameters of OD 8.4 / 13.8 / -3.50 and OS 8.4 / 13.8 / -4.00. The patient reported equal comfort and vision to the PureVision lenses. She was able to successfully adapt to these lenses, with no additional episodes of sharp pain or discomfort due to the recurrent erosions. Biomicroscopic examination of her corneas during the period of silicone hydrogel lens wear revealed stable geographic areas of negative staining. The patient reported that she was very pleased with the comfort and vision with these lenses, and that she was happy that the episodes of pain had stopped. She will continue to be monitored every 6 months.
Discussion:
Epithelial basement membrane dystrophy, also known as Cogan’s microcystic dystrophy and map-dot-fingerprint dystrophy, is a chronic bilateral corneal condition that has been reported to affect anywhere from 0.02% 1 to 42% 2 of the general population, though most sources report about 5-6% prevalence3, 4. EBMD consists of aberrant, sheet-like anterior basement membrane tissue that projects from the basement membrane into the epithelium. Maturing epithelial cells become trapped under the sheets of basement membrane, creating microcysts that can measure up to 1 mm in diameter. Areas of abnormally thickened basement membrane within the epithelium create the map-like or fingerprint areas commonly observed3. These areas of microcysts, maps and fingerprints create irregular areas of epithelial cell layers that result in an irregular corneal surface and spontaneous epithelial cell erosions. The corneal surface irregularities can cause blurry vision and are most easily seen in retroillumination on slit lamp examination. The spontaneous erosions can result in transient pain that can last minutes to days, depending on the severity of the erosion. It has been reported that EBMD, with or without trauma, is the most common cause of recurrent erosions5. However, patients with EBMD as a result of trauma are more likely to have recurrent erosions3, 6.
Treatment of recurrent erosions from EBMD depends on the severity of the case. Mild cases can be treated with lubricants and hypertonic saline drops during the day, and lubricating ointments at bedtime. Patching may help more severe cases. Bandage soft contact lenses can help more severe acute cases, especially when used on an extended wear basis. More invasive treatment options include stromal puncture, epithelial debridement, and phototherapeutic keratectomy3, 6.
Historically, the use of bandage contact lenses has been criticized and considered a secondary option due to the risk of microbial keratitis, particularly with overnight wear. With the introduction of silicone hydrogel soft contact lenses, much of the risk for complications, including microbial keratitis, has been reduced, particularly for limited amounts of overnight wear. In addition, Ciba Vision’s Focus Night & Day lens has received FDA approval for use as a therapeutic bandage lens, and is becoming a more commonly selected option for bandaging the cornea. Reports of the therapeutic use of silicone hydrogels have demonstrated their efficacy and relative safety as compared to traditional low-Dk bandage lenses when used for conditions such as recurrent erosions7, 8, 9.
This case illustrates the effective use of silicone hydrogel contact lenses in a case of mild recurrent epithelial erosions from EBMD. In this case, the lenses were prescribed on a daily wear regimen to minimize the recurrence of periodic episodes of pain due to mild erosions. Over the course of 4 years following refitting from gas permeable lenses, the patient has not had recurrence of pain from recurrent erosions. In cases where pain management, corneal healing, and corneal protection are needed, a silicone hydrogel contact lens should be considered a viable option.
References:
- Guerry D. Fingerprint lines in the cornea. Am J Ophthalmol 1950; 33:724-26.
- Werblin TP, Hirst LW, Stark WJ, Maumenee IH. Prevalence of map-dot-fingerprint dystrophy of the cornea. Br J Ophthalmol 1981; 65(6): 401-09.
- Laibson PR. Anterior Corneal Dystrophies. In: Krachmer JH, Mannis MJ, Holland EJ, eds. Cornea. St. Louis: Mosby-Year Book, Inc. 1997: 1033-42.
- Laibson PR. Microcystic corneal dystrophy. Trans Am Ophthalmol Soc 1976; 74: 488-531.
- Williams R, Buckley RJ. Pathogenesis and treatment of recurrent erosion. Br J Ophthalmol 1985; 69(6): 435-37.
- Reidy JJ, Paulus MP, Gona S. Recurrent erosions of the cornea: epidemiology and treatment. Cornea 2000; 19(6): 767-71.
- Lim L, Tan DTH, Chan WK. Therapeutic use of Bausch & Lomb PureVision contact lenses. CLAO J 2001; 27(4): 179-85.
- Montero J, Sparholt J, Mely R, Long B. Retrospective case series of therapeutic applications of Lotrafilcon A silicone hydrogel soft contact lenses. Eye & Contact Lens 2003; 29(2): 72-75.
- Kanpolat A, Ucakhan OO. Therapeutic use of Focus Night & Day contact lenses. Cornea 2003; 22(8): 726-34.
|



 Ronald K. Watanabe, OD, FAAO, Associate Professor, The New England College of Optometry, Chief, Cornea and Contact Lens Service, New England Eye Institute
Ronald K. Watanabe, OD, FAAO, Associate Professor, The New England College of Optometry, Chief, Cornea and Contact Lens Service, New England Eye Institute