As we see the last winter snowfalls, the days get warmer, and the nights draw out, those of us who live in the northern hemisphere, start thinking about spring. Spring is a wonderful time of the year; we can finally get into our gardens, get out on the golf course, and pursue our favourite outdoor activities. Unfortunately for some of our contact lens wearers it is a miserable time of the year, when their hayfever symptoms start and their tolerance to contact lenses drops.
Seasonal allergic conjunctivitis (SAC, commonly known as hayfever) is caused by an IgE-mediated or type 1 hypersensitivity. Here, the ocular allergic response is initiated when a particular antigen (normally pollen) dissolves in the tears and binds with immunoglobulin E (IgE) antibodies, which occupy the Fc receptors on conjunctival mast cells. Once the mast cells have been sensitised in this way, the patient needs to be exposed to the antigen once more for symptoms to emerge. When this happens the antigen bridges two of the IgE molecules attached to the conjunctival mast cells, and the mast cells are stimulated to degranulate (see Fig 1).
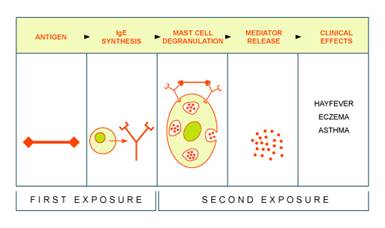 |
| Figure 1 - click to enlarge |
Degranulation of mast cells releases various mediators, producing a myriad of clinical signs and symptoms. These inflammatory mediators include histamine, neutral proteases, eosinophil-derived enzymes, complement proteins, interleukins, as well as a host of other cytokines. The release of these mediators into the tear film attracts leukocytes into the conjunctiva and is responsible for the immediate signs and symptoms we see with our contact lens patients. It should be noted that the majority of these inflammatory mediators, including IgE, are proteins. In addition to this, there is increased mucus secretion, which is believed to come from the goblet and non-goblet epithelial cells, and the mucus-secreting acinar cells of the lacrimal gland.
It has been estimated that 20% of the population have a family history of atopic disease, such as asthma, hayfever or eczema. The relevant IgE can be found in the tears and in the serum, so it is understandable that almost one person in 10 in the UK is affected by SAC. The airborne pollens which cause SAC vary throughout the season; in April to May, trees are responsible; in May to July the more common grass pollen is responsible; and by July to September, at the end of the season, moulds are often responsible.
Patients who develop SAC have classical signs of rhinitis: a runny and itchy nose which is sometimes blocked, sneezing, and watery itchy red eyes. When wearing contact lenses, the itchy red eyes become worse and vision becomes smeary; wearing times are reduced and swollen upper lids cause soft lenses to ride high (see Fig 2).
 |
| Figure 2 |
We know from the work of Jones et al. (1) that group IV hydrogel materials attract large amounts of lysozyme, but in the allergic eye there is no increase in the production of lysozyme so it is unlikely that lysozyme is responsible for many of the soiled lenses we see in contact lens practice in patients with SAC. We do know that there is an increase in the amount of protein in the allergic eye because of the inflammatory mediators that are released, and it can be assumed that these proteins, along with the increased production of mucus, forms a muco-protein deposit on the lens.
So will the new generation of silicone hydrogels improve our management of the contact lens wearing patient with SAC? The following case report illustrates how silicone hydrogels can alleviate many of the symptoms of contact lens wearing patients with SAC.
Case study
A 38 year old patient was wearing group II lenses every day for up to 16 hours. The patient details are as follows:
Spectacle prescription |
Contact lens prescription (alphafilcon A) |
R -2.75 / -0.25 x 90 6/6 |
R 8.70/ 14.2 / -2.75 |
L -2.75 / -0.25 x 90 6/6 |
L 8.70/ 14.2 / -2.75 |
The patient suffered from mild SAC most years, with rhinitis, for which he took Triludan®. Otherwise general health was good, with no medications or family history of systemic disease. Ocular health was good, with no history.
Subjective assessment
During the SAC season, the lens moved excessively; vision was variable, mucus strands were present and the eyes were itchy, particularly after lenses were removed. The patient was on a monthly disposable system with a PHMB preserved multipurpose solution, and was compliant.
Objective assessment
| Best visual acuity with lenses during the SAC season was R + L 6/7.5 (variable) |
| Biomicroscopy: |
grade 2 bulbar injection R + L |
| |
grade 2 tarsal hyperaemia |
| |
grade 1 tarsal papillae (macropapillae >0.3 mm) in zone 1 |
The cornea was clear with no signs of infiltrates.
Lenses were coated with translucent protein film and mucus strands.
Diagnosis
SAC with mild contact lens papillary conjunctivitis (CLPC) complicated by soiled soft contact lenses
Plan
Reducing the amount of muco-protein deposition on the lenses could well reduce the CLPC that he developed every hayfever season. With this is mind we switched him to high-Dk silicone-hydrogel lenses in an attempt to reduce the deposition.
The patient reported that switching to silicone-hydrogels made a vast improvement to both comfort and wearing times. The bulbar injection had reduced and upper lid eversion showed a reduction in hyperaemia and tarsal papillae. The lenses were no longer riding high and were centring well, with no visible deposition.
Discussion
Silicone-hydrogel contact lenses have been available in the UK for almost six years now, and without doubt have changed practitioners' perceptions about continuous wear. The literature is full of references pertaining to their high oxygen permeability and their virtual elimination of all hypoxic related adverse responses. Unfortunately, many practitioners see silicone-hydrogels as a extended/continuous wear lens, and if they're not involved with this modality see little point in keeping up-to-date with new developments.
The attributes of silicone-hydrogels is not confined to oxygen permeability alone; one of their greatest assets is the ability to attract less amounts of protein such as lysozyme. Patients who have SAC, such as in the case study presented here, should benefit greatly from wearing a silicone-hydrogel, if only during the hayfever season. Indeed, the patient in this case study was so pleased with the silicone-hydrogels that he is now wearing them on a 30 day continuous wear modality.
We are now entering a period in contact lens history, where the old HEMA-based lenses are being phased out, and are being replaced with silicone-hydrogels not only for continuous wear but also for the very large daily wear market. We still have a lot to learn about the way the surfaces of these new lenses interact with the tear film, but anecdotally these lenses work very well with our long-suffering hayfever patients.
Reference
1. Jones L., Senchyna, M., Louie D., Schickler, J., (2001) A comparative evaluation of lysozyme and lipid deposition on etafilcon, Balafilcon and lotrafilcon contact lens materials. Invest ophthalmol Vis Sci., 42 (s 593), 3186
|



 Jonathon Walker
Jonathon Walker