A 48 year old female was referred for complicated contact lens fitting on October 12, 2006 after penetrating keratoplasty in her left eye for a long standing Fuch’s Dystrophy. The surgery was performed elsewhere in June 2005. A running suture remained and the surgeon planned to keep the suture in place for another year. She initially presented to her local optometrist for contact lens fitting in June 2006. After several failed attempts of rigid gas permeable {RGP} lens fittings she was referred to me for consultation. The lenses tried prior to referral for complicated contact lens management included standard and reverse geometry RGP lens designs which all dropped to the lower limbus and trapped bubbles centrally. The patient also reported she could not tolerate the lenses longer than two hours, or they popped out frequently. Because of the difficultly in fitting the left eye with a contact lens, the referring optometrist and surgeon were planning to wait until the sutures were removed to refit the left eye, however the right eye was rapidly visually deteriorating from progressing Fuch’s dystrophy, and her vision was no longer satisfactory in either eye.
At the first visit with me baseline data for the left eye included:
Manifest Refraction +9.00 -4.00 X 045 (20/40)
Simulated Keratometry: 38.58@149/33.99@059
Biomicroscopy: running suture intact, graft clear yet sunken centrally and raised wound at graft-host interface (Figure 1)
Topography: Figure 2
 |
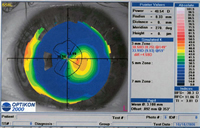 |
Figure 1 |
Figure 2 |
click to enlarge |
click to enlarge |
As can be seen from Figures 1 and 2, the graft was irregular, excessively flat, and depressed relative to the best fit reference sphere and the raised wound margins. Because of the elevation differential of the central cornea compared to the mid-periphery, a traditional RGP design trapped bubbles centrally. My fitting approach was to change the graft contour by adding a high plus powered silicone hydrogel soft lens as a piggyback lens beneath an RGP.
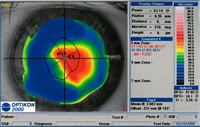
The first silicone hydrogel lens attempted was an 8.7mm +7.00 galyfilcon A (Acuvue Advance). The topography over this soft lens was then repeated (Figure 3) which revealed significant steepening centrally and an improved “fitting surface”. The RGP diagnostic lens fit over this surface was:
 |
 |
Figure 3 |
Figure 4 |
click to enlarge |
click to enlarge |
Base Curve: 8.44mm
Diameter 11.2
Optical Zone: 9.4mm
Power: -1.00
Peripheral Curve System: standard periphery
Design/Material: Dyna Z Intralimbal in Menicon Z
Over-refraction +0.75 1.00 X015 (20/25)
This lens exhibited central corneal clearance, low edge lift and temporal decentration, yet this piggyback fitting approach showed promise. The following modifications were made to the piggyback lens system ordered:
Soft lens:
8.4 mm +7.00 senofilcon A (Acuvue Oasys)
RGP:
Base Curve: 8.65mm
Diameter 10.8mm
Optical Zone: 8.8mm
Power: +0.25
Peripheral Curve System: flat periphery
Design/Material: Dyna Z Intralimbal in Menicon Z
On October 31, 2006, this patient returned for dispensing of the piggyback combination. The RGP exhibited a good central fluorescein pattern with faint touch centrally, pooling in the paracentral area, and adequate edge lift. However, the lens still remained decentered supero-temporally although there was full pupillary coverage. (Fig 4) The over-refraction was +1.50 (20/25).
The following RGP was re-ordered:
Base Curve: 8.65mm
Diameter 11.2mm
Optical Zone: 8.8mm
Power: +1.75
Peripheral Curve System: flat periphery
Design/Material: Dyna Z Intralimbal in Menicon Z
In this piggyback lens system, the RGP still decenters slightly temporally but superiorly, and is thus comfortable for the patient with no excessive lens loss and provides the patient excellent vision while awaiting penetrating keratoplasty in the right eye.
Discussion:
Post-keratoplasty fitting is often challenging with a variety of graft contours posing difficulty with traditional RGP fitting approaches. One such challenging graft contour is the oblate shape, which is often associated with a raised graft-host interface in a recently transplanted graft.
Soft lenses have limited potential in full thickness post-keratoplasty eyes. Usually the astigmatism is irregular, and thus soft lenses will not adequately visually rehabilitate the eye. Even if the astigmatism was regular, most contact lens fitters shy away from low Dk soft lenses because of the risk of graft edema and neovascularization. Since silicone hydrogel lenses have become available in toric and high powered prescriptions, the door has opened up for many post-keratoplasty patients to wear soft lenses if their prescription is available.
This case posed a challenge from a geometric standpoint. A high plus powered soft lens was used to transform the excessively flat central graft to a more prolate shape. Prior to the availability of silicone hydrogel lenses in high powered prescriptions, this would not have been possible. As stated above, I feel a low Dk soft lens in a thick high plus design was contraindicated in such a patient due to potential hypoxic complications. However with this high Dk soft and RGP lens combination, hypoxia is not expected to be a concern.
The lens materials chosen were based on the highest Dk availability in both categories for the given prescription. Although lotrafilcon A has a higher Dk value than senofilcon A, the highest plus prescription available is +6.00, which may have also worked but was not attempted.
Since this experience, I have been using other high powered silicone hydrogel lenses to improve the graft contour after keratoplasty. For example, after penetrating keratoplasty for keratoconus, it is not uncommon to encounter an oblate cornea with an excessively steep host inferior cornea. I routinely have difficulty in fitting RGP lenses in such patients when the inferior cornea exhibits lens edge standoff. I have successfully used high minus silicone hydrogel lenses (such as -7.00) to produce a more spherical shape in these patients which improves the physical fitting relationship of the RGP lens.
|



