In the United States, FDA approval for Intacs to treat keratoconus was obtained in August, 2004. Keratoconus, which causes thinning of the cornea, affects up to 300,000 people in the United States [1]. The Intacs approval allows intrastromal ring inserts to be used for the reduction or elimination of myopia and astigmatism in patients with keratoconus where functional vision is difficult with contact lenses or spectacles. The inserts may defer the need for a corneal transplant for some patients and ideally allow for functional spectacle-corrected vision or easier contact lens fitting.
Potential patients for this therapy must be 21 years of age or older, with no history of autoimmune or immunodeficiency disease. They must have nearsightedness and astigmatism as a result of keratoconus and be unable to achieve adequate vision correction with contact lenses or glasses. Patients must also have clear central corneas that are not excessively thin (approximately no less than 450 micrometers at the incision site, although thinner corneas may be considered). Contraindications are pregnancy or nursing, any medical conditions or medications that could lead to delayed corneal healing, or any previous herpetic ocular infection.
The intrastromal corneal ring inserts act as passive spacing elements that shorten the arc length of the anterior corneal surface and therefore flatten the cornea [2]. The flattening effect of the rings may be greater in thinner, softer keratoconic corneal tissue. The goal of treatment is to reshape keratoconic corneas with two Intacs of the same or different thicknesses (refractive effect is modulated by the Intacs thickness which ranges from 0.25 mm to 0.45 mm in 0.05 mm steps) [3]. In the United States, surgeons are limited to implanting 0.25 mm, 0.30 mm, and 0.35 mm inserts [4]. The segments are applied to lift the usually inferior ectasia and to flatten the soft keratoconic tissue, which decreases the asymmetric astigmatism. Generally a thicker ring is placed in the usually thinner inferior area and a thinner ring is placed in the superior region for more asymmetrical or oval cones; rings of equal thickness may be used for central or global cones. The channels for Intacs insertion can be made using a mechanical keratome or a femtosecond laser (Intralase) [5].
CASE STUDY
Patient AV, a 21 year old female was first diagnosed with keratoconus at age 15. She had a history of seasonal allergies. Her mother had advanced keratoconus at an early age leading to a penetrating keratoplasty in one eye. Patient AV complained of decreasing vision during the past year.
November 2000
| Subjective findings: |
|
| Uncorrected DV VA: |
OD 20/100, OS 20/50. |
| Corrected VA: |
OD -.50 -3.00 x 45 20/70, |
| |
OS -.50 – 1.50 x 165 20/25. |
Corneas were clear of opacities and striae, exhibiting mild thinning only. Topography revealed a large inferior cone OD with moderate central steepening OS (see Figure 1).
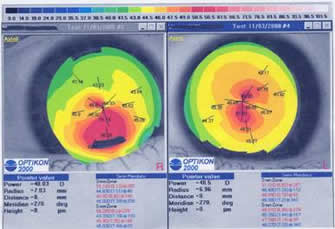 |
| Figure 1- Topography OU at presentation - click to enlarge |
Visual acuity with gas permeable lenses was 20/25 OD, 20/20 OS. The patient successfully adapted to gas permeable lens wear at that time and was lost to follow-up.
January 2003
The patient returned for a visit complaining of decreased vision OU and contact lens intolerance. Best spectacle acuity at this time was OD 20/200, OS 20/60. Topography revealed significant steepening and keratoconic advancement OU (see Figure 2). At this time she was refit with Rose K design in the Boston ES material.
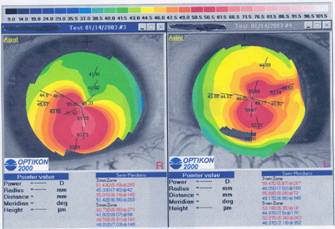 |
| Figure 2 - Topography OU after gas permeable lens wear - click to enlarge |
Parameters were:
OD: BC 6.7mm, TD 8.7 mm, STD periphery, -4.25D, 0.14 mm ct 20/30
OS: BC 6.9mm, TD 8.7 mm, STD periphery, -4.75D, 0.14 mm ct 20/40.
The lenses fitted well but due to continued discomfort she was also dispensed 8.3 mm, -2.00D two-week disposable hydrogel lenses for use as a piggy-back system. She wore these piggy-back lenses successfully for 1.5 years.
February, 2005
The patient returned in 2005 for a follow-up visit. During November, 2004, without consulting our office, she obtained Intacs surgery for her right eye. She was unhappy with the results and wished a contact lens refitting. Her uncorrected OD VA was 20/200. A refraction of -1.25 – 1.50 x 90 gave 20/80-2 VA. The left eye continued to wear the previous piggy-back design with 20/40 VA. Topography revealed flattening of the cornea from the Intacs (see Figure 3) versus the previous topography. Because of previous discomfort problems and good success with the fit of the disposable hydrogel, she was refit with a daily wear silicone hydrogel lens of -2.00D allowing for easy lens handling and excellent comfort. The silicone hydrogel lens in the chosen lens power has a Dk/t close to 87 units*. Silicone hydrogels are now preferred for piggy-back fittings due to the excellent oxygen transmissibility and material characteristics.
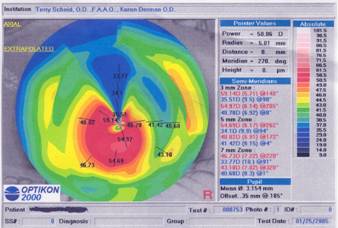 |
| Figure 3 - Topography OD, post Intacs - click to enlarge |
Measurement of corneal topography over the silicone hydrogel lens showed further corneal flattening (see Figure 4). Increasing the minus of the silicone hydrogel will flatten the surface further although not in an entirely predictable manner for a keratoconic cornea. She was refit successfully with an Apex Aspheric gas permeable design (X-Cel Contacts) with a base curve of 7.5 mm, TD 9.3 mm, Medium periphery, -0.50D, 0.17 mm ct, in Boston XO material. This material has a published Dk of 100 barrers. With this combination her VA was 20/30 with excellent adaptation.
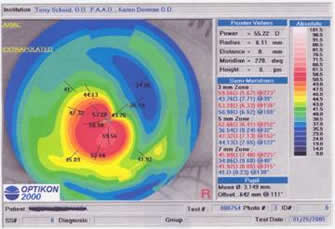 |
| Figure 4 -Topography OD, with silicone hydrogel lens - click to enlarge |
Calculating Dk/t of a piggyback lens system
Calculating the oxygen transmission of a piggyback system involves Ohm’s Law. The resistance of the two lenses in series is the sum of the resistance offered by each. Transmissibility is the reciprocal of resistance, so to determine the resistance of two lenses in series, you need to add the reciprocal of their transmissibilities [6]. In addition there is a tear film layer between the two lenses that contributes a small additional resistance beyond that occurring with just one lens on the cornea. The resistance of this layer is approximately 0.003 or a Dk/t of 333.
For the piggyback lens system in this case, the Boston XO GP lens had a Dk of 100 and centre thickness of 0.17 mm, giving a Dk/t of 58.8. The reciprocal of this Dk/t is a resistance of 0.01695. The Dk of the silicone hydrogel was 60 barrers and in the utilized lens power, Dk/t was nearly 87. The reciprocal of this is a resistance of 0.01149. The total resistance of the two lenses and the tearfilm layer between these lenses is 0.0314, which means that the effective transmissibility of this piggyback system was approximately 32 units.
Conclusion
In the presented case Intacs insertion in the right cornea resulted in fitting a significantly flatter gas permeable base curve (7.5 mm versus previous 6.7 mm) with a significantly lower gas permeable dioptric power (-0.50D versus previous -4.25D). A piggy-back fit utilizing a silicone hydrogel lens greatly enhanced patient comfort and adaptation. Practitioners should consider piggy-back fitting irregular corneas as needed using high-Dk gas permeable and silicone hydrogel lenses. The impact of using the highest-Dk lens materials available on the total oxygen transmissibility of a piggyback lens system is provided in the table below.
Lens |
Dk
(barrers)
|
Centre thickness |
Dk/t (units*)
|
Resistance |
RGP |
163 |
0.17 mm |
95.9 |
0.0104 |
Silicone hydrogel |
140 |
0.08 mm |
175 |
0.0057 |
Tear Film |
|
|
|
0.003 |
TOTAL |
|
|
52 |
0.0191 |
| *units = x 10-9 (cm/sec) (ml O2/ml x mm Hg). |
References:
1. Addition Technology Receives FDA Approval for Intacs to Treat Keratoconus. Press release from Addition Technology, August 4, 2004 www.getintacs.com
2 . Burris TE, Baker PC, Ayer CT, et. al.. Flattening of Central Corneal Curvature with Intrastromal Corneal Rings of Increasing Thickness. J Cataract Refract Surg 1993; 19S: 182-187.
3. Colin J, Cochener B, Savary G, et. al.. Intacs Inserts for Treating Keratoconus: One Year Results. Ophthalmology Vol. 108; 8: 1409-1414.
4 . Colin J, Velou S. Current Surgical Options for Keratoconus. J Cataract Refract Surgery 2003; 29: 379-386.
5. Charters L. Laser Channels Improve Accuracy in Corneal Inserts Placement. Ophthalmology Times; March 2005: 38.
6 . Personal correspondence 1989 with Dr. Irving Fatt, Univ of California Berkeley College of Optometry, and 2005 with Dr. William J Benjamin UAB Birmingham College of Optometry. |



 Terry Scheid, OD
Terry Scheid, OD