|
Every now and then, after taking a history, you have to take a deep breath – in preparation for the ensuing examination which you know will not be straightforward. These challenging patients can test your capabilities and demand your time, but when you reach a solution, it certainly makes all your efforts worthwhile.
Mrs B, a 54 year old female, reported decreased distance and near vision with her 6 year old soft conventional contact lenses. She was unaware of the brand of lenses and had not seen an eyecare practitioner for over 5 years. Mrs B had worn contact lenses for 23 years and admitted to not having a current pair of glasses, forcing her to wear her lenses 7 days a week, 16 hours a day.
She disinfected her lenses with ReNu MultiPlus solution. Mrs B reported no prior infections or injuries to her eyes and her general health was good, with no medications taken.
Visual acuities with her contact lenses were R 6/30- and L 6/30. The fit was satisfactory, but the lenses were discoloured with a light brown tinge.
Her spectacle refraction was R -16.75DS and L -15.25/-0.75x115 giving acuities of R 6/12= and L 6/12=. A near addition of +1.75DS enabled N5 print to be read.
The simulated K readings on the Medmont E300 corneal topographer were:
| R 7.79@102 |
L 7.87@43 |
| 7.95@12 |
7.92@133 |
Slit lamp examination, not surprisingly, showed 3600 corneal neovascularisation in both eyes. This hypoxic sign was more pronounced superiorly, as shown in Figure 1.
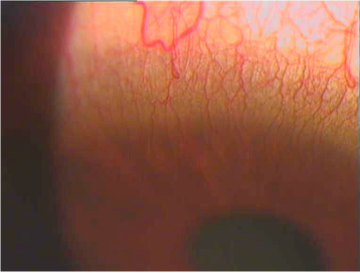 |
Figure 1, corneal neovascularisation superiorly |
Figure 1. Corneal neovascularisation superiorly
Mrs B was prescribed distance glasses and given the options of reducing soft contact lens wear to a part-time basis or being refitted with RGP lenses.
The following month, Mrs B returned for an RGP lens fitting. She chose to try monovision rather than alternating bifocal lenses or distance lenses with reading overspectacles. She is right eye dominant.
RGP tricurve lenses made of Boston XO material were delivered with the following parameters:
R 7.9/9.5/-14.25, BOZD 7.5, PC +0.7(0.6), +1.3(0.4)
L 7.9/9.5/-12.00, BOZD 7.5, PC +0.7(0.6), +1.3(0.4)
She could see 6/7.5= with her right eye, N5 with her left eye and managed 6/7.5 binocularly. Both lenses fit well with good centration and edge clearance.
Mrs B had difficulty learning insertion and removal of these RGP lenses and abraded the superior cornea of her left eye during the delivery appointment. She returned the next day to review the epithelial defect which had almost completely resolved. However, Mrs B was very anxious and apprehensive about proceeding with RGP lenses.
She was prepared to resume wearing soft conventional lenses, to be worn on a part-time basis. Sensing the potential risk that she would return to full-time wear, she was offered the possibility of trialing disposable silicone hydrogel lenses with overspectacles as the highest BVP available was -12.00DS.
Her ocular refraction was R -13.50DS and L -12.50/-0.50x115 and she was given PureVision lenses (8.6/14.0/-12.00) to wear in both eyes.
Mrs B was very happy with the comfort and vision with these lenses and was not concerned that the dominant right eye was in fact corrected for near. There was no option of increasing the BVP for the right eye.
At a review two months later, her right lens enabled her to read N5 print and 6/15 at distance, improving to 6/7.5 with an over-refraction of -1.50DS. Her left eye could resolve 6/9.5, improving by two letters with an over-refraction of -0.50DS. Binocularly, Mrs B managed 6/7.5= and N5. She declined distance overspectacles, thrilled that her vision was already much better than with her original lenses.
The PureVision lenses fitted well and the neovascularisation was diminishing. She was wearing the lenses 7 days a week, 8 hours a day, replacing them monthly and disinfecting with AQuify MultiPurpose Solution.
Two years later in 2007, Mrs B continues to wear PureVision lenses successfully. Nowadays, there are other options for high myopes who require silicone hydrogel contact lenses.
Gelflex Laboratories has a custom silicone hydrogel lens called Hygel, available in powers of -10.00DS to +10.00DS in 0.25DS steps and ±10.50DS to ±15.00DS in 0.50DS steps. Cylinder powers are available up to -4.00DC with any axis between 10 and 1800.
There is a choice of 5 base curves (8.0, 8.3, 8.6, 8.9, 9.2) and 3 diameters (14.3, 14.8, 15.3). Its water content is 53% and is only available as a clear lens currently which is not ideal for high ametropes who prefer a handling tint. It has a Dk of 53, suitable for daily wear and annual replacement is advised.
An alcohol-based surfactant cleaner is recommended to reduce the build-up of lipid deposits1 which tend to be more of an issue with silicone hydrogel lenses. [2] With the return of MiraFlow Daily Cleaner back onto the market, this lens may soon gain popularity amongst patients whose prescriptions fall outside the disposable range.
Ciba Vision will soon be introducing their custom silicone hydrogel lens called O2 OPTIX Custom. It will be available in powers of -20.00DS to +20.00DS in 0.25DS steps, with 3 diameters in a range of base curves. This daily wear, quarterly replacement lens has a Dk of 82, water content of 32% and comes in a light green handling tint. [3]
It won’t be long before more custom silicone hydrogel contact lenses make their appearance as conventional hydrogel lenses become a thing of the past.
This case highlights two important points:
- It is often difficult to convert a long-term soft contact lens wearer to RGP lenses. We are fortunate now to have the option of silicone hydrogel lenses to manage these patients with hypoxic signs.
- Monovision worked well for this patient even though her dominant eye was given the near correction - purely by circumstance and not by choice. It was definitely worthwhile trying this approach which provided a much better alternative to her original situation, both visually and physiologically.
References
- Ghormley NR, Jones L. Managing lipid deposition on silicone hydrogel lenses. Contact Lens Spectrum 2006; 21(1): 21.
- Cheung S, Cho P, Chan B, Choy C, Ng V. A comparative study of biweekly disposable contact lenses: silicone hydrogel versus hydrogel. Clin Exp Optom 2007; 90 (2): 124-131.
- http://www.specialty-lenses.com/custom/overview.html Accessed 5 July 2007
|



