Manuscript Review
Validation of grading scales for contact lens complications
Efron N, Morgan PB, Katsara SS Ophthal Physiol Opt. 2001, 21:
17 - 29.
Clinical grading scales provide a means by which practitioners
can assess the severity and evaluate the progression of complications
associated with contact lens wear. A number of authors (1,2,3)
have described the use of scales for grading adverse responses
such as corneal staining, conjunctival/bulbar redness and contact
lens-associated papillary conjunctivitis (CLPC).
| |
|
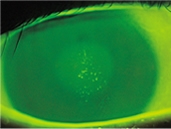
Macropunctate Corneal Staining
(CCLRU Grade Type 2)
Click on image to magnify |
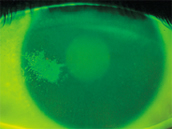
Patch Corneal Staining (CCLRU
Grade Type 4)
Click on image to magnify |
In clinical research and practice it is common to use subjective
ratings of the degree of severity and change of clinical conditions
that commonly occur. Many authors have described the need for
a grading system to possess high reliability and also the power
to discriminate accurately. Such scales should be capable of being
administered quickly and simply.
Chong et. al. (4) examined the repeatability of discrete and
continuous anterior segment grading scales. They suggest that
grading scales that are coarse generally allow less sensitivity
in the detection of meaningful clinical changes and point out
that practitioners often overcome this limitation by adopting
half-point scales, or by assigning plus and minus symbols next
to an integer scale. They also suggest that by increasing the
number of intervals to make the grading scale finer may reduce
the degree of concordance between repeated measurements of the
same clinical event (5). Finer scales have the advantage of
being more sensitive to detect clinical difference (5).
This review examines a paper that describes the features of
a number of different grading systems for use during contact
lens wear (6).
The authors examined four illustrative contact lens grading
scales and described them as the 'Efron', 'Annunziato', 'CCLRU'
and 'Vistakon' systems. The images depicted in the Efron and
Annunziato systems were painted by the ophthalmic artists Terry
Tarrant and Monte Lay respectively, whereas those images represented
in the CCLRU and Vistakon scales were developed from a collection
of clinical photographs.
The aim of the study was to validate the four grading systems
by way of documenting differences in their grading precision
and reliability and to offer advice to practitioners of the
expected performance of each system in a clinical setting. The
authors chose the three complications that are common to each
of the grading scales i.e. corneal staining, ocular redness
and papillary conjunctivitis. Thirty images presented on a computer
monitor of each of the complications were independently graded
by 13 optometrists to the nearest 0.1 grading unit using each
of the four systems. This same test was repeated some two weeks
later using a different randomised sequence.
This study attempted to define the precision and reliability
of the clinical grading techniques. Precision is defined as
the closeness of agreement between independent test results
obtained under specific conditions whereas reliability is the
ability of the grader to give similar results time after time.
The authors posed two questions:
- 'Do some observers grade significantly higher or lower
than other observers?'
- 'How consistently can an observer judge a given non-varying
condition on two occasions?'
The result of this study demonstrated that there are differences
in the use of the four grading systems with respect to precision.
Such differences need to be taken into account when comparing
grading scores obtained using the different scales. This study
also indicates that there are significant differences in grading
precision between observers. The authors suggest using a correction
factor to normalise the grading scores. The use of a training
program to standardize the clinicians will also increase the
degree of concordance between observers using such grading scales.
The overall reliability result was 0.63 grading scale units,
giving 95% confidence limits of ± 1.23 grading scale
units. The authors suggest that a change or difference in severity
of greater than 1.2 grading scale units, when detected using
any of the four systems investigated in the study, can be taken
to be both clinically and statistically significant. It is important
to remember that this study was conducted using untrained observers.
This reinforces the need for all clinicians participating in
research studies to undergo a rigorous training program to understand
the application and implementation of any type of grading scale.
The study indicated that all four grading scale systems are
validated for clinical use however the authors offer the following
advice:
- Clinicians are advised to consistently use the same grading
system
- Practitioners should develop an awareness of their own grading
reliability
Grading scales offer the clinician the most effective way of
monitoring the health of an eye wearing a contact lens. They
allow for an accurate means of detecting change that can occur
during lens use and provide the practitioner with the necessary
information to intervene to minimize the risk of a chronic adverse
reaction to the contact lens. Ideally, prior to contact lens
wear, the baseline data for a range of clinical variables should
be collected and then monitored throughout the course of the
study or clinical assessment period.
References
1. Løfstrøm T, Andersen JS, Kruse A (1998). Tarsal
abnormalities: a new grading system. Contact Lens Assoc Ophthalmol
J. 24: 210 - 215.
2. Mackinven J, McGuinness CL, Pascal E, Woods R (2001). Clinical
grading of the upper palpebral conjunctiva of non-contact lens
wearers. Optom Vis Sci. 78: 13 - 18.
3. McMonnies CW, Chapman-Davies A (1987). Assessment of conjunctival
hyperaemia in contact lens wearers. Part 1. Am J Optom Physiol
Opt. 64: 246 - 250.
4. Chong T, Simpson T, Fonn, D (2000). The repeatability of
discrete and continuous anterior segment grading scales. Optom
Vis Sci. 77: 244 - 251.
5. Bailey IL, Bullimore MA, Raasch TW, Taylor HR (1991). Clinical
grading and the effects of scaling. Invest Ophthalmol Vis Sci.
32: 422 - 432.
6. Efron N, Morgan PB, Katsara SS (2001). Validation of grading
scales for contact lens complications. Ophthal Physiol Opt.
21: 17 - 29.



 NICOLE
CARNT - BOptom 1980 UNSW MSc 1995 UNSW
NICOLE
CARNT - BOptom 1980 UNSW MSc 1995 UNSW