|
Over the past 3 years, more than 200 hypermetropic patients
have been fitted with both Night and Day and Purevision lenses
in my practice, predominantly in monovision mode. In some cases,
there has been a relatively rapid increase in plus power, past
that normally expected for the age and refractive error of the
patient. This “hyperopic creep” has some interesting
clinical aspects, and raises some interesting questions as to
the effect of the lens material and design on corneal shape.
A review of the patient files shows that an unexpected increase
of greater than +0.50D occurs in the first year of lens wear in
approximately 12% of hyperopic patients whose previous records
show stabilization of refractive error. Greater refractive change
(=> 1.00D) associated with induced astigmatism occurs in approximately
3% of patients seen.
Of interest are the following clinical observations:
1. The time of onset appears to be variable, from weeks to
months.
2. The eye with the highest plus lens (the reading eye) is the
more likely to be affected.
3. The presenting complaint is increased difficulty with close
work.
4. Cessation of lens wear results in a return to baseline refraction
within 10 days, associated with a return to baseline corneal
topography.
5. Changing the base curve of the lens, or changing from Night
and Day to Purevision or vice versa has no effect: the increased
hypermetropia returns within 1-2 weeks.
6. A change form Extended wear to daily wear has no effect.
7. A return to hydrogel lenses results in a return to baseline
refraction and topography.
A typical case is that of JC, a 58 y.o. female, who had successfully
worn Acuvue lenses on a daily wear monovision schedule for 5 years,
with little or no change to her distance Rx of R&L +1.75D,
and a mild increase in the Left near vision lens from +3.75 to
+4.00D the year before.
She was fitted with silicone hydrogel lenses to the following
Rx:
OD +1.75 (6/5)
OS +4.00 (n.5)
Extended wear was initiated in November 2001, and was uneventful.
The patient returned in April 2002 with symptoms of blurred near
vision. The distance vision remained unchanged at 6/5 with an
over-refraction of plano.
The near vision could not be improved with the addition of low
plus lenses, so the lens was removed and refraction performed.
The result was:
Rx +4.25/-1.50 x 125 (6/6).
The patient was advised to cease lens wear, and returned 1 week
later. The refraction had returned to baseline, with no astigmatic
component present.
The patient was returned to lens wear, but this time with a different
brand of silicone hydrogel lenses lenses (OD +1.75, OS +4.25)
and after 2 weeks, returned with the same problems with near work.
Once again, refraction showed an increase in both hypermetropia
and astigmatism to +3.75/-1.00 x 120.
Lens wear was again ceased for 2 weeks, and refraction and topography
once again returned to baseline. Due to the unwanted changes,
the patient returned to daily wear disposable lenses (Acuvue).
Review over the following year has not resulted in any refractive
change.
|
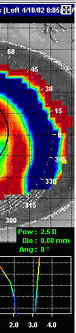
| Figure 1. The top left plot shows
the cornea following lens removal. Note the “red ring”
of corneal steepening at the 6.00mm zone. The inferior left
map shows the cornea after 1 week of no lens wear. The subtractive
map (right) shows that the cornea has steepened by 2.50D since
lens wear was ceased. Also note the irregularity of the central
pupil zone resulting in the induced astigmatism. The “blue
ring” show where the cornea has flattened following
cessation of lens wear. |
A subtractive tangential power topography map of the cornea immediately
on lens removal and following a return to baseline is shown in
Figure 1. Note the apparent steepening of the central cornea following
cessation of silicone hydrogel wear. The analogy is that lens
wear resulted in a marked degree of central corneal flattening.
The topography map on the top left hand side bears some remarkable
similarities to those seen following orthokeratology lens wear
(see Figure 2). The central corneal flattening is associated with
a ring of mid-peripheral steepening. The difference map in figure
1 shows this area is having flattened (blue ring) following cessation
of lens wear.
|
| Figure 2 . A post- wear topography
map of a cornea following orthokeratology. Note the flattening
of the central cornea, and the mid-peripheral “red ring”
of steepening. A similar effect appears in post-wear hypermetropic
silicone hydrogel lens wear. |
Reverse geometry lenses produce a change in corneal shape due
to the differences in tear layer fluid forces acting under the
lens. They do not compress the cornea into a new shape, but rather
tend to use negative force or suction in order to “draw”
the corneal epithelium into a shape similar to the back surface
geometry of the lens.
The higher modulus of silicone hydrogels (especially in the plus
lens design) may mean that they do not, like high water content
soft lenses. “wrap” onto the cornea and mimic its
shape. They may, in fact, have a relatively deep tear layer trapped
between the lens and the corneal surface that, due to the aspheric
back surface of the lens and relatively flat base curve to cornea
fitting relationship is deeper at the edge of the optic zone than
in the centre. This is similar to the tear layer shape caused
by reverse geometry lenses. It is interesting to postulate that
the increased plus seen in some patients may be due to corneal
flattening as a result of the same type of squeeze film forces
present in reverse geometry lenses, albeit to a much lesser degree.
The recent interest in tear layer thickness research under silicone
hydrogels may shed more light on the topic.
In conclusion, an interesting patient presented for review 3
weeks ago. The initial refraction was -11.00D sph. After 6 weeks
of continuous wear of a –10.00D silicone hydrogel lens,
he returned complaining of blurred distance and near vision. Over-refraction
with the lens in place was +2.00D. Refraction without the lens
in-situ was -8.75D. The lens was changed to -8.00D, which,
after 2 weeks required a change back to – 10.00D. Topography
plots have been taken, and it will be interesting to see if the
reduction in myopia occurs again.
Silicone hydrogels cause refractive changes in some patients,
with the changes appearing to be greater in hypermetropes, and
being totally due to some form of corneal molding by the lens.
Perhaps the decrease in minus seen in previous soft lens wearers
may also be influenced by alterations to corneal shape.
To quote and old saying….”curioser and curioser”.
|



 John
Mountford, FAAO, FCLSA, FVCO, Dip. App. Sc
John
Mountford, FAAO, FCLSA, FVCO, Dip. App. Sc