When visiting the optometrist or ophthalmologist, a patient will encounter the process of refraction. A distance prescription derived from refraction is designed to correct two types of refractive errors: spherical and cylindrical errors. But what if the refractive error of the eye is not well characterized by sphere and cylinder alone? One subset of individuals whose visually significant refractive error is often more complex than traditional sphere and cylinder is found in patients with keratoconus. Correction of sphere and cylinder alone in this population can leave behind significant uncorrected refractive errors in the visual system. The impact on the image forming properties of the eye is demonstrated in Figure 1, which shows a simulated retinal image of a letter chart for a keratoconus subject where spherical and cylindrical errors have been perfectly corrected. In this case, the non-sphero-cylindrical refractive errors remain, and are present at such a level that they continue to degrade retinal image formation.
 |
| Figure 1: A simulation of the retinal image of a letter chart for an individual with keratoconus with perfect sphere and cylinder correction. As can be seen, the acuity chart remains blurred due to the presence of non-sphero-cylindrical refractive errors. |
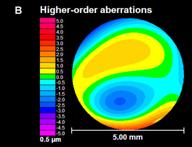
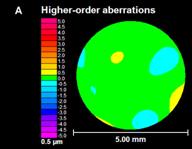
The use of the Zernike polynomial has become increasingly common in the ophthalmic community and has been adopted as a standard for describing ocular aberration in the eye. Its utility can be seen in the fact that the Zernike polynomial can describe not only sphere and cylinder (lower order aberrations), but also these other aberrations (higher order aberrations) that play a role in image degradation. The ability to quantify this more complete set of errors is now possible with a variety of clinical technologies that allow for the quick, objective quantification of the optical defects of the eye. One such technology used to quantify these optical errors is the wavefront sensor. Figure 2 shows two color-coded maps derived from wavefront sensor data that describe the higher order aberration (non-sphero-cylindrical errors) measured in a normal eye (Figure 2A) and a keratoconic eye (Figure 2B). These maps demonstrate the optical defects that would remain if the eyes were perfectly corrected for sphere and cylinder. At these scales, a majority of the map in Figure 2A is green, representing a relatively flat wavefront. However, the map in Figure 2B displays a much larger variation in color. This variation signifies the presence of higher order aberration in this individual keratoconic eye in a greater quantity than the normal eye shown in Figure 2A.
Many clinicians are familiar with wavefront sensing due to its current use with state-of-the-art refractive surgery platforms. However, the wavefront sensor is finding expanded clinical relevance as a diagnostic instrument in evaluating eyes that suffer from elevated levels of optical distortion, such as keratoconus. And researchers and clinicians are becoming increasingly interested in applying the information recorded by the wavefront sensor to the design of a wavefront-guided soft contact lens (WGSL).
|
| Figure 2: Higher order aberration (HOA) maps of two eyes. Fig 2A reports data for a normal eye and Fig 2B reports data for a keratoconic eye. This keratoconic eye exhibits elevated HOA compared to this normal eye. |
Conceptually, a WGSL is similar in nature to a traditional soft contact lens with the exception that the optics of the WGSL lens are designed based on the more complete description of refractive error found in wavefront sensor measurements. The optical zone of the WGSL may contain lower order aberration correction of sphere and cylinder, as well as higher order aberration correction for aberrations such as coma, spherical aberration, trefoil, etc. Correction of higher order aberration in this manner would provide a method to directly target the more complete set of the optical defects that lead to reduction in the image forming capabilities of the highly aberrated keratoconic eye. And such technology would make soft lenses more applicable to the keratoconus population than current sphero-cylindrical soft lens designs. Implementation of this custom technology in the form of silicone hydrogel lenses may also be an area for future research.
While attractive conceptually, the successful, widespread deployment of WGSLs presents the patient, clinician, researcher and industrial partner with many challenges. To date, wavefront sensors are not universally available in the clinical setting. However, their numbers and capabilities are increasing and will continue to increase as clinicians and scientists find more utility for the information they produce. Another challenge comes in the nature of the WGSL as presented here, which is highly custom, meaning that a given lens design is based on an individual patient’s wavefront measurement and would apply only to that individual patient. This is in contrast to the current method of prescribing the bulk of soft contact lenses, which combines discrete levels of correction such that a handful of lenses will apply to the largest number of individuals. Additional challenges present in the fact that WGSLs can be very sensitive to movement, and significant movement of a WGSL can reduce visual performance. Finally, the fact that keratoconus is a progressive disease process will ultimately leave any decision on the appropriateness of this technology for a given patient to the clinician.
To date, multiple research groups have demonstrated that the design, manufacture and evaluation of WGSLs is possible, and these demonstrations fuel the continued hope that WGSLs will provide clinicians with yet another tool in the care of those that currently suffer from highly aberrated optics, such as patients with keratoconus.
|



 Jason D. Marsack obtained the PhD degree in Physiological Optics from The University of Houston College of Optometry (UHCO) in 2007, the MS degree in Biomedical Engineering from The University of Texas in 2001 and the BS degree in Computer Engineering from Texas A&M University in 1998. He has served as a Research Assistant Professor at UHCO for the past 2 years, where his work has focused on development of custom wavefront-guided soft contact lenses for the highly aberrated eye.
Jason D. Marsack obtained the PhD degree in Physiological Optics from The University of Houston College of Optometry (UHCO) in 2007, the MS degree in Biomedical Engineering from The University of Texas in 2001 and the BS degree in Computer Engineering from Texas A&M University in 1998. He has served as a Research Assistant Professor at UHCO for the past 2 years, where his work has focused on development of custom wavefront-guided soft contact lenses for the highly aberrated eye.