| INTRODUCTION |
Features of the design and material properties of silicone hydrogel
lenses mean that proper fitting is vital in order to provide optimum
patient comfort and to minimize the risk of mechanically-induced
adverse responses. Trial lens fitting should always be done before
the commencement of daily or continuous wear with silicone hydrogel
lenses and, if any problem with fit is observed, an alternative
design or product should be tried. As we know initial comfort during
trial fitting greatly influences the patient's perception of contact
lenses1 , 2 and may
affect their ultimate success. For this reason, increasing the probability
of achieving an optimal lens fit with the first trial lens will
ultimately benefit both the patient and the practitioner.
Historically, central corneal curvature, as measured by keratometry,
has been used to predict the optimum soft contact lens base curve,
particularly for thicker lenses. Other parameters including corneal
diameter, asphericity and sagittal height have been shown to be
more useful when predicting the fit of thinner lens designs3.
Hydrogel trial lens fitting has become somewhat simplified since
the introduction of thinner designs. Many lenses are now only available
in one or two base curves, and most practitioners rely on the approach
of fitting one-fit disposable lenses to achieve an acceptable fit
in a high percentage of cases.
Silicone hydrogel lens materials, as described in last month's
editorial, differ significantly from conventional soft lenses.
The increased stiffness of the materials lessens the degree to
which they shape themselves to the cornea, compared to other soft
lenses. As a result silicone hydrogel lenses are less "forgiving"
to marginal fits. There may also be a tendency for the material
to 'flute' (this is a
buckling of the lens edge due to excessive edge lift) at the edges
of the lens if the fit is not optimal.
The two types of silicone hydrogel lenses currently on the market
are available in the parameters listed below (Table 1). Many myopic
and hyperopic patients can be successfully fitted with these lenses
regardless of whether the lenses will be worn on a daily or continuous
wear basis. Currently these lenses are only available in spherical
prescriptions and as silicone hydrogel lenses do not "mask"
astigmatism despite their higher modulus, only patients with less
than a dioptre of astigmatism should be considered. 
| Proprietary
Name |
PureVision |
Focus®
NIGHT & DAY™ |
| Manufacturer |
Bausch &
Lomb |
CIBA Vision |
| Ct (@ -3.00D) mm |
0.09 |
0.08 |
| Diameter mm |
14 |
13.8 |
| Base Curve(s) mm |
8.6 |
8.4, 8.6 |
| Power D |
+6.00
to -9.00
-0.50 to -6.00 (0.25 steps)
+0.25 to +6.00 (0.25 steps)
-6.50 to -12.00 (0.50 steps)
|
+6.00
to -10.00
-0.25 to -8.50 (0.25 steps)
+0.25 to +6.00 (0.25 steps)
-8.50 to -10.00 (0.50 steps)
|
| Table 1:
Parameters available for silicone hydrogel materials. |
|
| HOW TO ASSESS LENS FIT |
|
Lens fitting characteristics should be assessed using conventional
techniques and measurements. A period of 10 to 15 minutes after
insertion is recommended for lens settling prior to assessment.
A slit lamp biomicroscope at low magnification, employing diffuse
illumination, should be used for careful examination of the lens
centration and corneal coverage. Direct focal illumination with
a wide illuminating beam (0.5-2.0mm) can be used to assess lens
movement in primary and superior gaze and to assess alignment
of the lens particularly around the periphery to ensure that there
is no edge stand off. Varying the width or length of the beam
can aid in measuring the lens movement or alternatively a reticule
eyepiece may be utilised.
The tightness of lenses
may be assessed with a push up test5.
In this test the lens is dislodged by gently pushing upwards on
the lower eyelid margin against the lower edge of the contact
lens and then releasing the lid. The resistance to decentration,
or tightness, is rated according to the speed at which the lens
returns to a central position. The rating is a percentage scale
where 0% represents the lens being held by lid tension only (that
is, it falls from the cornea immediately the lower lid is released)
and 100% represents no movement on attempting to decentre the
lens. Thus a lens rated at 0% is too loose, and a lens at 100%
is too tight, or is bound.
|
| WHAT CONSTITUTES A GOOD FIT? |
|
The general principles for a well fitting silicone hydrogel lens
are no different from those used for conventional soft lenses.
The lens should cover the entire cornea and limbus and remain
approximately central on the cornea in all gaze positions. Sufficient
lens movement is required to maximise tear exchange and to encourage
the removal of debris and bacteria from under the lens.
The push-up test5 should give a
tightness rating of 40-45% (slightly loose). Typically lens movement
with silicone hydrogels is greater than observed with conventional
thin soft lenses, averaging 0.3mm - 0.5mm in the primary, and
up to 0.75mm in the superior gaze positions. Lenses that "flute"
will cause discomfort and lens awareness. If a lens does flute,
a steeper base curve or different lens type is indicated.
|
| WHAT CONSTITUTES A POOR FIT? |
|
Lenses, which decentre, move excessively or do not provide complete
corneal coverage should be avoided to prevent corneal desiccation
or limbal chafing. As mentioned previously, the increased stiffness
of silicone hydrogel materials makes them less prone to conform
to the corneal surface, meaning that the physical lens to cornea
curvature relationship is more critical to successful fitting.
A phenomenon that is observed more often with silicone hydrogel
lenses than conventional soft lenses is lens 'fluting'6.
It may occur constantly or intermittently and can be most readily
detected by observing the lens edge moving over the temporal limbal
area near the lower lid. Lenses exhibiting fluting usually cause
a foreign-body like discomfort or increased lens awareness. In
extreme cases the lens will ride on the lower lid margin causing
a varying degree of discomfort (Figure 1). Unfortunately fluting
does not reduce with wear, the patient will not adapt to the lens
awareness or discomfort induced and if observed, an alternate
base curve or design must be evaluated.
| |
| Figure 1: Extreme case of lens
fluting seen in a small percentage of potential wearers. |
|
| THE USE OF FLUORESCEIN IN ASSESSING
LENS FIT |
|
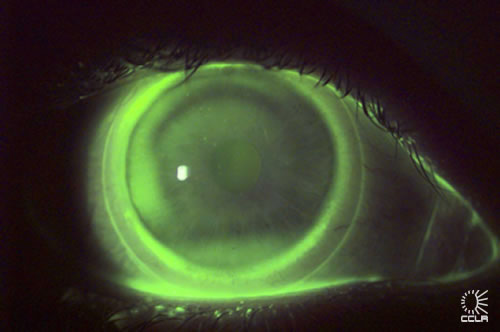
High molecular weight fluorescein dye or fluorexon may also be
used to assess the static and dynamic lens fitting characteristics
of silicone hydrogel lenses. A cobalt blue excitation filter and
yellow barrier filter can improve the contrast of the fluorescein
pattern (Figure 2). For optimal visibility the dye should be instilled
on the back surface of the contact lens before insertion of the
lens. Minimal dosage is of importance because higher amounts of
the dye can cause stinging which results in excessive tearing
and therefore an inaccurate assessment. Conventional fluorescein
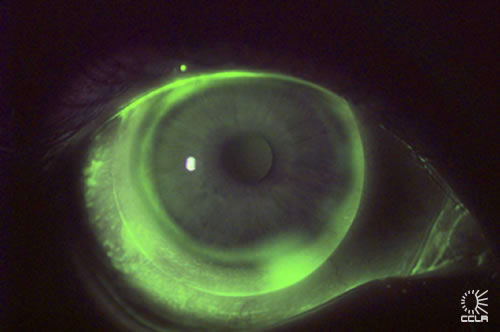
may be used to assess fit in a similar manner. Fluting (Figure
3), particularly if minimal or intermittent will be more easily
observed with this technique.
| |
| Figure 2: Well fitted silicone
hydrogel lens observed with fluorexon, cobalt blue excitation
filter and yellow barrier filter. |
| |
| Figure 3: Fluting is more easily
observed with fluorexon, cobalt blue excitation filter and
yellow barrier filter. |
|
| SELECTION OF BASE CURVE BASED ON
CORNEAL CURVATURE |
|
The PureVision lens is currently only available in one base curve
- 8.7mm. This base curve has been shown to fit a wide range of
corneal curvatures, with average keratometry readings of flatter
than 40.00 D (8.4mm) to steeper than 48.00 D (7.0mm). The distribution
of average keratometry readings for a group of 2250 eyes successfully
fitted with PureVision lenses is shown in Figure 4. (Bausch &
Lomb data)
|
| Figure 4: Distribution of K readings
from clinical studies: PureVision™. |
The Focus Night & Day lens is available in two base curves,
8.4mm and 8.6mm. Figure 5 shows the distribution of keratometry
data along the steep meridian for eyes fitted with each lens base
curve (CCLR data). A clinically useful criterion that indicated
the need for the 8.4 lens was a steep K of >45.50 D (<7.4mm).
 |
| Figure 5: Distribution of steep
keratometry readings for eyes dispensed in 8.6 and 8.4 mm
base curve lenses: Focus® NIGHT & DAY™. |
|
| THE RELATIONSHIP BETWEEN LENS FIT
AND COMFORT |
|
In a clinical trial conducted at the CCLR, the effect of lens
base curve on subjective comfort during trial fitting5
was investigated. Subjective discomfort during trial fit with
the flatter lens was determined to be a strong indication of the
need for a steeper base curve since the 8.4 lens resulted in significant
improvement in comfort among subjects who reported poor comfort
with the 8.6 lens. Figure 8 shows that subjects with steeper eyes
among this subset had a large improvement in comfort when changing
to the steeper lenses.
 |
| Figure 8: Mean "settled"
subjective comfort scores during trial fitting of 8.6 mm and
8.4 mm base curve Focus® NIGHT & DAY™ lenses,
for eyes requiring the 8.4 mm base curve lenses. |
From this study we were able to conclude that subjective comfort
was vastly improved with the steeper base curve lenses in the
steeper range of corneas.
Some patients currently wearing soft lenses may experience more
lens awareness, at least initially, when being refitted with silicone
hydrogel lenses. It is important for the practitioner to be aware
of this and advise the patient accordingly.
|
| CONCLUSION |
Optimum fitting can significantly improve the chances for successful
lens wear. Fitting procedures for silicone hydrogel lenses are the
same as for conventional soft lenses, and trial lens fitting is
essential. Particular attention with silicone hydrogels should be
paid to centration, movement and the possibility of lens fluting.
Subjective comfort levels may be more important with silicone hydrogel
lenses during the fitting procedure.
|
|
REFERENCES
1. Efron N, Brennan NA, Currie JM, et al. Determinants
of the initial comfort of hydrogel contact lenses. Am J Optom
Physiol Opt 1986; 63:819-23.
2. McMonnies CW. The critical initial comfort
of soft contact lenses. Clin Exp Optom 1997;80:53-8.
3. Young G. Ocular sagittal height and soft
contact lens fit. J Brit Contact Lens Assoc 1992;15:45-9.
4. Dumbleton K, Chalmers R, Bayer S, Fonn D,
McNally J. Lens base curve and subjective comfort with silicone
hydrogel continuous wear lenses. Optom Vis Sci 2001; 78 (12s):
227.
5. Young G, Holden BA, Cooke G (1993): Influence
of soft contact lens design on clinical performance. Optom Vis
Sci 70: 394-403
6. Clinical performance of silicone hydrogel
lenses. In: Sweeney DF, ed. Silicone Hydrogels: the rebirth of
continuous wear contact lenses. Butterworth-Heinemann, Oxford
2000; chap. 5. |
|



 Kathryn
Dumbleton - BSc (Hons), Uni of Wales1984 MCOptom 1985,
MSc Uni of Waterloo 1988
Kathryn
Dumbleton - BSc (Hons), Uni of Wales1984 MCOptom 1985,
MSc Uni of Waterloo 1988