The Physical and Clinical Characteristics
of Silicone Hydrogel Lenses: How They Work?
Kathryn
Dumbleton - BSc (Hons), Uni of Wales1984 MCOptom 1985,
MSc Uni of Waterloo 1988
Senior Researcher
Centre for Contact Lens Research (CCLR)
University of Waterloo, Ontario, Canada
Introduction
Silicone hydrogel lenses are a made
from an innovative group of extremely oxygen permeable contact
lens materials. The development of these materials arose from
the desire to eliminate the hypoxic responses known to occur as
a result of wearing conventional hydrogel materials on an extended
wear basis.
It was proposed that combining the properties of silicone and
hydrogel materials would offer many advantages including the comfort
and wettability of hydrogels and the high oxygen transmissibility
of silicone.
Silicone hydrogel materials differ considerably from the silicone
rubber (elastomer) lenses used for therapeutic or paediatric applications.
Although silicone-elastomeric lenses offered exceptional oxygen
transmission and durability, a number of major limitations are
associated with their use in clinical practice. As fluid is unable
to flow through the lens and the lens surfaces are hydrophobic,
binding to the ocular surface is very likely.
Binding of a silicone rubber (elastomer)
lens
Materials
All contact lens materials are polymers.
The constituent monomers which comprise the polymers determine
the physical and chemical properties of the materials. Repeating
chains of monomers are arranged in patterns with cross-linking
between the polymer chains to afford strength and further govern
the characteristics of the lens materials. The monomers commonly
employed in contact lens materials include N-vinyl pyrrolidone
(NVP), methacrylic acid (MA) and poly-2-hydroxyethyl methacrylate
(pHEMA). These polymers allow the lens materials to absorb and
bind water.
In silicone hydrogel materials, silicone rubber is combined with
conventional hydrogel monomers. The silicone component of these
lens materials provides extremely high oxygen permeability, while
the hydrogel component facilitates fluid transport and thus lens
movement. Unfortunately, this process or combination is not without
difficulty and it has therefore taken some considerable time for
these materials and designs to come to fruition. The process of
combining these monomers has been likened to efforts of combining
oil with water, while maintaining optical clarity[1].
An additional impediment to the development of these contact
lens materials relates to the decreased wettability, increased
lipid interaction and accentuated lens binding inherent in silicone
based materials. Therefore a technology referred to as “gas
plasma surfacing” is employed in order to render the surfaces
hydrophilic[2].
Poor wetting of a silicone rubber
(elastomer) lens
How they work
Detailed explanations of the development
of silicone hydrogel materials for contact lenses[1,3]
and their polymer chemistry[4] have been described
previously. The following account is intended to provide a brief,
simplified overview for practitioners.
Contact lens materials must permit the transmission of both oxygen
and ions. One approach which may be used to achieve this goal
involves the incorporation of two “phases” into the
materials. Phase separation occurs when the interconnections between
the chemically similar molecules in the material are stronger
than the adhesive connections between them and the different molecules.
This approach to material development was historically avoided
because it usually resulted in an opaque material which would
be unsuitable for contact lenses. However, techniques have been
developed in which the phase separation is limited, such that
the phase size is far shorter than the wavelength of light, resulting
in optically clear materials[4].
CIBA Vision’s Focus Night and Day? material, lotrafilcon
A, employs such a biphasic or two channel molecular structure.
The fluorosiloxane phase facilitates the storage and transmission
of oxygen and the hydrogel phase transmits water and oxygen, allowing
good lens movement. The two phases work concurrently to allow
the co-continuous transmission of oxygen and ions. Lotrafilcon
A is comprised of a fluoroether macromer co-polymerised with the
monomer trimethyl-siloxy silane (TRIS - used in the preparation
of RGP materials) and the solvent N,N-dimethyl acrylamide (DMA)
in the presence of a diluent. The resultant silicone hydrogel
material has a water content of 24% and an oxygen permeability
(Dk) of 140 barrers. Lenses are manufactured from lotrafilcon
A using a standard industry molding process and then the surfaces
are permanently modified in a gas plasma reactive chamber to create
a permanent, ultrathin (25nm) continuous hydrophilic surface.
Bausch and Lomb’s PureVision? material, balafilcon A, is
a homogeneous combination of the silicone containing monomer Polymethylsiloxane
(a vinyl carbamate derivative of TRIS) co-polymerized with the
hydrophilic hydrogel monomer N-vinyl pyrrolidone (NVP). This silicone
hydrogel material has a water content of 36% and a Dk of 110 barrers.
Cast molded balafilcon A lenses are surface treated in a gas plasma
reactive chamber[2] which transforms the silicone
components on the surface of the lenses into hydrophilic silicate
compounds. Glassy silicate “islands” result and the
hydrophilicity of these areas "bridges" over the underlying
hydrophobic balafilcon material.
The flow of oxygen and fluids through the lenses is not impeded
by these surface modifications. Both surface treatments are an
integral part of the lens and are not surface coatings that can
be easily “stripped” away from the base material. Silicone
hydrogel lenses have also been reported to have extremely low
protein deposition[5].
Oxygen Transmissability
and Corneal Health
A sufficient oxygen supply is required
in order to maintain corneal integrity and to provide defence
against infection. The minimum requirements for oxygen transmissibility
(Dk/t) of extended wear contact lenses in order to prevent overnight
hypoxia-induced edema was estimated to be 87 x 10-9 (cm x ml O2)/(s
x ml x mmHg) by Holden and Mertz in 19846.More recently a level
of 125 x 10-9 (cm x ml O2)/(s x ml x mmHg) has been reported as
a requirement to prevent stromal anoxia[7].
Traditional contact lenses have relied on water to carry the
oxygen through the lens. This has been a limiting factor, since
100% water has a Dk of only about 80 barrers. As a result, conventional
hydrogel lens materials do not deliver sufficient oxygen during
extended wear and a number of clinical signs of chronic hypoxia
may occur. Conventional high-water lenses needed to be made thicker
than their low water counterparts resulting in relatively low
Dk/t values. Consequently, thicker high-water content lenses and
thinner low-water content lenses deliver approximately the same
amount of oxygen to the central cornea. It is the close relationship
between water content and oxygen permeability that has impeded
hydrogel lens material development for extended wear for more
than 20 years.
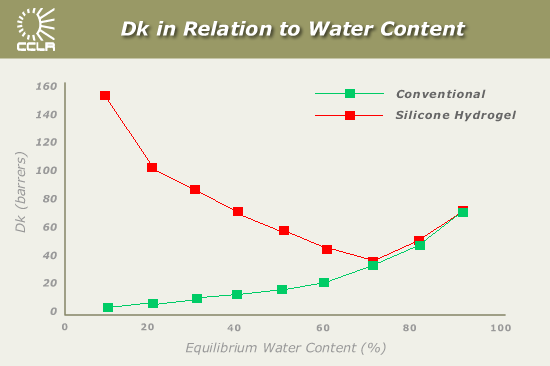
In silicone hydrogel materials the oxygen is transmitted through
the silicone component of the lens material, resulting in a dramatic
increase in the oxygen permeability. Pure silicone rubber has
a Dk of 400 to 600 barrers and this provides silicone hydrogel
materials with Dk/t values of 110 to 175, which is 6 times more
permeable than conventional hydrogel contact lenses. Figure 1
is redrawn from Brian Tighe’s chapter in Silicone Hydrogels[1]
and demonstrates the Dk of these materials compared with conventional
materials, in which the Dk is directly related to the water content
of the lens material.
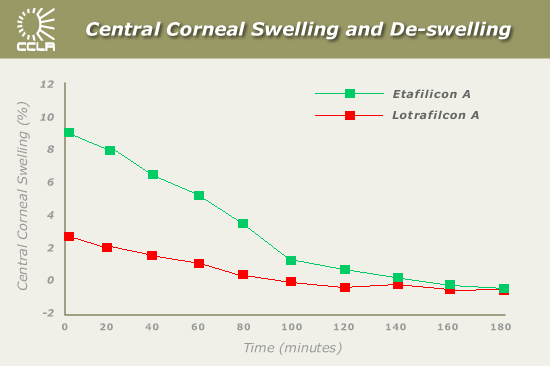
As a result of the increased oxygen availability, studies conducted
at the CCLR have found overnight edema levels with the new generation
materials to be similar to the levels seen with no lens wear and
to be far lower than those measured with commercially available
disposable soft lenses[8]. Figure 2 demonstrates
the degree of central corneal swelling upon eye opening for eyes
wearing etafilcon A (Acuvue?) and lotrafilcon A (Focus Night and
Day?) lenses.
Central corneal swelling induced by an etafilcon A lens on eye
opening was significantly higher than with a lotrafilcon A lens
(8.7 ± 2.8% vs. 2.7 ± 1.9%, p<0.00001). The de-swelling
profiles following lens removal were much quicker for the lotrafilcon
A induced corneal swelling (100 minutes) than for etafilcon A
induced swelling, which took almost twice as long to return to
baseline levels.
In a similar study, the overnight central corneal swelling induced
by balafilcon A lenses (PureVision?) was found to be 2.8 ±
2.0% compared to 8.7 ± 2.7% with a 70% water content lens
(Dk/t = 22)9.
Ionic and Hydraulic Permeability
and Lens Movement
The transport of fluid and ions through
contact lenses is crucial for the provision of essential nutrients
and removal of waste products and debris. The flow of water through
the lens is also necessary for on-eye lens movement, comfort and
wettability. It is the hydrogel component of lens materials that
is responsible for these processes.
In homogenous silicone hydrogel materials such as balafilcon
A, while the oxygen permeability increases, the hydraulic permeability
decreases with decreasing water content. This is because fluids
and ions are transported through the hydrogel component of the
lens material. A minimum sodium ion and hydraulic permeability
of 0.2 x 10-6 cm2sec-1 has been reported to be required for lens
movement1. A balance therefore has to be reached between maximising
oxygen transmission while still allowing sufficient hydraulic
flow to prevent hydrophobic binding of the lens to the cornea.
In biphasic co-continuous silicone hydrogel materials such as
lotrafilcon A, the oxygen and fluid permeability are “uncoupled”
allowing a much greater level of hydraulic and ionic permeability
than would be available through a polyHEMA with an equivalent
water content. As a result, lenses made from this material display
adequate lens movement while still benefiting from the additional
oxygen permeability afforded with a water content of 24%. In the
case of the balafilcon A material, a water content of 36% provides
a hydraulic permeability which actually corresponds with that
normally offered by a 40% water content lens. This suggests that
there may also be some degree of phase separation of the material.
Mechanical
Properties and Lens Stiffness
Lens adhesion is also a factor of
material elasticity. Pure silicone materials are extremely elastic
and tend to adhere to the cornea with a “suction effect”.
The material elasticity of the currently marketed silicone hydrogel
lenses is much less and fortunately approaches that of HEMA. This
further helps to prevent lens adhesion and promote movement and
tear flow beneath the lens.
Silicone hydrogel lenses are however much “stiffer”
than their conventional hydrogel counterparts. It is this property
that gives the lenses their excellent handling characteristics.
The modulus, stiffness or rigidity of the materials is 110 - 120
g/mm2 (1.1 - 1.2 MPa)1 which is over twice that of polyHEMA and
nearly four times greater than the HEMA-methacrylic acid components
of the etafilcon A material (Acuvue?). As a consequence, the “stiffer”
material does not drape over the cornea as easily. When silicone
hydrogel lenses are too loose, the result is often a lens that
exhibits edge lift or slight fluting that causes foreign-body
like discomfort to the patient10. 8.2% of post- dispensing discontinuations
with Focus Night and Day? lenses have been attributed to poor
fit[11]. Following the introduction of a further
steeper base curve for this lens type, a recent study has shown
that for trial fitting assessment and subjective comfort, 98%
of the patients in the trial could be satisfactorily fitted with
a choice of an 8.4 or 8.6 mm base curve[12].
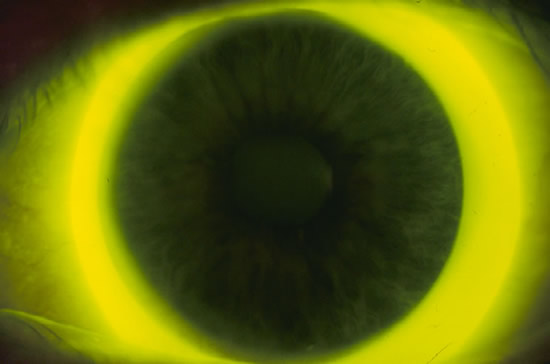
Fluting of a silicone
hydrogel lens as seen in a small percentage of potential
wearers
Handling properties
of silicone hydrogel materials are excellent
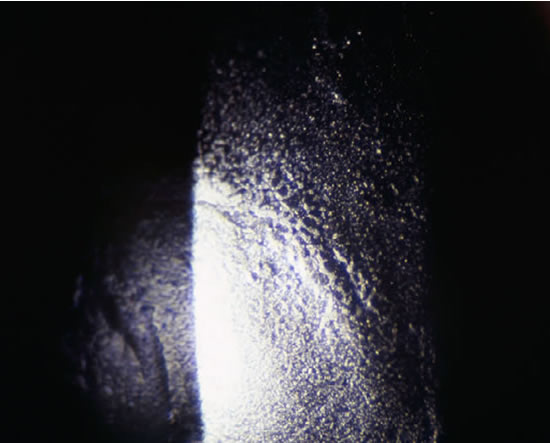
The increased stiffness likely contributes to the formation of
mucin balls beneath the lenses with overnight wear[13].
It may also be a factor in the formation of superior epithelial
arcuate lesions (SEALs) in some patients. SEALs have been reported
to occur more frequently with silicone hydrogel materials than
conventional hydrogel lenses[14,15]
Summary
Table 1 summarises the differences between the
two commercially available silicone hydrogel materials and compares
them with the Acuvue? lens material.
Table 1: Characteristics
of Novel and Conventional Lens Materials
Proprietary
Name
PureVision™
Focus
Night & Day™
Acuvue™
Manufacturer
Bausch
and Lomb
CIBA-Vision
Vistakon
Ct (@ -3.00D)mm
0.09
0.08
0.07
Water Content
36%
24%
58%
Dk
99
140
22
Dk/tx10-9@ 35oC
110
175
31
Surface Charge
Surface
slightly ionic
Surface
slightly ionic
Surface
highly ionic
Surface Treatment
Plasma
oxidation, producing glassy islands
25nm
plasma coating with high refractive index
No treatment
“Stiffness”
(g/mm2)
110
120
35
FDA Group
III
I
IV
Monomers
NVP +
TRIS-VC
DMA +
TRIS + siloxane macromer
HEMA
+ MA
USAN
balafilcon
A
lotrafilcon
A
etafilcon
A
DMA (N,N-dimethylacrylamide); HEMA (poly-2-hydroxyethylene methacrylate);
MA (methacrylic acid); NVP (N-vinyl pyrrolidone); TRIS-VC (tris-(trimethylsiloxysilyl)
propylvinyl carbamate).
New silicone hydrogel materials are currently being developed
and modifications made to those currently available. Future designs
may benefit from decreases in modulus (and consequently stiffness)
and changes to the manufacturing process in order to increase
the rate of production at a lower cost. These changes will offer
the practitioner and patient a wider choice of lens materials
and designs in order to achieve successful continuous wear.
References
1. Tighe B. Silicone hydrogel materials - how do they work ? in
Silicone Hydrogels: The Rebirth of Continuous Wear Contact Lenses,
D. Sweeney, Editor. Oxford, Butterworth-Heinemann. 2000, pp 1 -
21.
2. Grobe GL. Surface engineering aspects of silicone-hydrogel lenses.
Contact Lens Spectrum (suppl). August 1999, 14-17.
3. Künzler JF. Silicone-based hydrogels for contact lens application.
Contact Lens Spectrum (suppl). August 1999, 9-11.
4. Nicholson PC and Vogt J. Soft contact lens polymers: an evolution.
Biomaterials. 2001; 22: 3273-3283.
5. Jones L, Senchyna M, Louie D, Schickler J. A comparative evaluation
of lysozyme and lipid deposition on Etafilcon, Balafilcon and Lotrafilcon
contact lens materials. Invest Ophthalmol Vis Sci 2001; 42: s593
#3186.
6. Holden B, Mertz G: Critical oxygen levels to avoid corneal edema
for daily and extended wear contact lenses. Invest Ophthalmol Vis
Sci 1984; 25: 1161-1167.
7. Harvitt DM and Bonanno JA. Re-evaluation of the oxygen diffusion
model for predicting minimum contact lens Dk/t values needed to
avoid corneal anoxia. Optom Vis Sci 1999; 76(10):712-719.
8. Fonn D, du Toit R, Simpson TL, Vega JA, Situ P, Chalmers RL.
Sympathetic swelling response of the control eye to soft lenses
in the other eye. Invest Ophthalmol Vis Sci 1999; 40: 3116-21.
9. MacDonald K, Fonn D, Richter D, Robboy M. Comparison of the physiological
response to extended wear of an experimental high Dk soft lens versus
a 38% HEMA lens. Invest Ophthalmol Vis Sci 1995; 36: S310.
10. Sweeney DF et al. Clinical performance of silicone hydrogels.
in Silicone Hydrogels: The Rebirth of Continuous Wear Contact Lenses,
D. Sweeney, Editor. Oxford, UK, Butterworth-Heinemann,2000, pp 90
- 149.
11. Montero Iruzubieta J, Nebot Ripoll JR, Chiva J, Fernandez OE,
Rubio Alvarez JJ, Delgado F, Villa C, Traverso LM: Practical experience
with a high Dk lotrafilcon A fluorosilicone hydrogel extended wear
contact lens in Spain. CLAO J 2001; 27: 41-6.
12. Dumbleton KA, Chalmers RL, Bayer S, Fonn D, McNally J. Lens
base curve and subjective comfort with silicone hydrogel continuous
wear lenses. Optom Vis Sci; 78 (12s).
13. Dumbleton KA, Jones LW, Chalmers RL, Williams-Lyn D and Fonn
D. Clinical characterization of spherical post-lens debris associated
with lotrafilcon high Dk silicone lenses. CLAO 2000; 26 (4): 186
– 192.
14. Dumbleton K, Fonn D, Jones L, Williams-Lyn D, Richter D (2000).
Severity and management of contact lens related complications with
continuous wear of high Dk silicone hydrogel lenses. Optom Vis Sci
2000; 77 (12s): 216.
15. Holden BA, Stephenson A, Stretton S, Sankaridurg PR, O'Hare
N, Jalbert I, Sweeney DF: Superior epithelial arcuate lesions with
soft contact lens wear. Optom Vis Sci 2001; 78: 9-12.
All rights reserved, copyright 2002 - 2007 siliconehydrogels.org



 Kathryn
Dumbleton - BSc (Hons), Uni of Wales1984 MCOptom 1985,
MSc Uni of Waterloo 1988
Kathryn
Dumbleton - BSc (Hons), Uni of Wales1984 MCOptom 1985,
MSc Uni of Waterloo 1988