Another marker, perhaps the most clinically
useful, is the observation of epithelial microcysts. Microcysts
are small, irregularly shaped high refractive inclusions that
form in the basal layers of the epithelium and move towards
the anterior surface of the cornea.
| |
| Figure
2. Corneal Microcysts (courtesy Vision Cooperative Research Centre (VisionCRC) Grading
Scales) |
The technique for observing epithelial microcysts uses retro-illumination.
The cornea is scanned with a 1mm wide slit beam on a slit-lamp
biomicroscope. A magnification of at least 16x is required with
marginal retro-illumination. Once observed, magnification is
increased to 20-40x while keeping the inclusion centred in the
beam and confirming that it shows reversed illumination as demonstrated
in Figure 3. Microcysts are typically 10-50 microns in diameter
and appear similar to micropunctate corneal staining.
| |
| Figure 3. Observation of Unreversed
and Reversed Illumination (courtesy IACLE) |
Relatively low numbers of microcysts are observed in patients
wearing silicone hydrogels if they are new to contact lens wear
or have been wearing these lenses for some time (several months
or longer). This is because, as has been demonstrated previously
(6), the oxygen transmissibility of lenses is inversely proportional
to the number of microcysts seen.
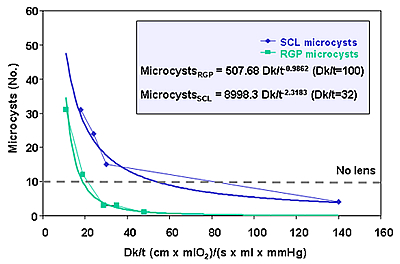 |
| Figure 4. Relationship between
microcyts and Dk/t for RGP and soft lenses (adapted from
"Silicone Hydrogels: the rebirth of continuous wear contact
wear" ed. Sweeney, DF) |
The number of microcysts is generally less than 10, a number
commonly seen in non-lens wearers and with daily wear of lenses.
Large number of microcysts however will be found in a significant
proportion of our patients that we transfer from low Dk lenses
particularly if worn on an extended wear basis, to high Dk SCLs.
In these patients, as has been reported by Keay and colleagues
(7), a spike or rebound effect will be observed with large numbers
of microcysts observed in the cornea for up to one month after
refitting. These large numbers of microcysts are seen to be
spread across the cornea or they have been noticed to aggregate
in a ring in the corneal mid-periphery. As microcysts move to
the anterior surface of the cornea, areas of negative staining,
or black spots, may be observed (best observed after instillation
of fluorescein using a cobalt blue illumination with a Wratten
yellow filter).
 |
| Figure 5. The typical trend
in microcyst numbers when moving patients from low Dk
to high Dk materials (adapted from "Silicone Hydrogels:
the rebirth of continuous wear contact wear", ed. Sweeney,
DF) |
Such a trend has also been observed when patients are discontinued
from low Dk extended wear. It has been suggested that the rebound
is related to re-oxygenation of the corneal surface resulting
in recovery of epithelial metabolism and so clearance of extra-cellular
debris trapped in the deeper basal layers of the epithelium.
We have also had the opportunity in our long-term studies to
monitor the levels of microcysts in our high Dk patients over
a number of years and with patients on both a 6 and 30 night
continuous wear schedule. We have observed no shift or increase
in the low numbers of microcysts observed across time and nor
have we seen any differences in the levels of microcysts observed
with either a 6 or 30 night wear schedule.
When observing the corneal epithelium it is important also to
ensure that microcysts are differentially diagnosed from the
many other presentations with which they may be confused. The
table below adapted from Keay et al (7) details a number of
conditions that can have a similar appearance to microcysts
and the main distinguishing feature by which to differentiate
them from microcysts.
Table 2: Differential diagnosis with other epithelial events
| |
<Size (µm) |
Appearance |
Cause |
| Recurrent corneal erosion
|
<15 to 100
|
Clear cysts
|
Trauma often unknown
|
| Microcystic edema
|
<20 to 50
|
Clear cyst surrounding epithelial
haze, > 200
|
Inflammatory origin
|
| Epithelial infiltrates
|
<100 to 500
|
Granular, dense centre
|
Chemotactic stimulus
|
| Vacuoles
|
<20 to 50
|
Round, bubble-like, unreversed
illumination
|
Hypoxia
|
| Mucin balls*
|
<< 100
|
Spherical balls
|
Surface interaction between lens
and cornea
|
| Punctate corneal staining
|
<10 to 50
|
Fine opaque dots, positive stain
|
Epithelial trauma (e.g. toxic
or dehydration)
|
| Microcysts
|
<10 to 50
|
Small, irregular-shaped dots;
reversed illumination (negative stain)
|
Hypoxia
|



 Deborah
Sweeney - BOptom (UNSW) 1980 PhD (UNSW)
1992
Deborah
Sweeney - BOptom (UNSW) 1980 PhD (UNSW)
1992