A CLINICAL LOOK AT DAILY WEAR WITH SILICONE
HYDROGEL LENSES
Advancements in contact lens technology
allow clinicians to solve more and more of our contact lens
wearing patients' problems. One of the most useful tools to
be developed in recent years is Silicone Hydrogel lenses (CIBA
Vision's Focus Night & Day
and Bausch & Lomb's PureVision Lenses). The benefits of these
lenses are clear in theory. Higher oxygen transmission 1-3 should
benefit most corneas and lead to improved ocular surface health
during lens wear 4;5 . The other characteristics of
the lenses which make them different include the stiffness of
the materials3 , lens design and lower water content. All these
features may contribute to more successful lens wear. The good
news is that with silicone hydrogel lenses the theory often translates
into clinical reality when the lenses are used to solve problems
and even as a lens of first choice.
AS A LENS OF FIRST CHOICE:
Some practitioners believe that the benefits of the
silicone content of these lenses make silicone hydrogel lenses
the first choice for all new fits because the oxygen benefits
of the lenses may reduce complications in the future4;5 . Certainly
for extended or continuous wear patients, the oxygen benefits
must make these the lens of choice6 . I have used silicone hydrogel
lenses principally in the daily wear modaility and I wanted to
share my clinical experiences with these lenses with the readers.
In my practice, these types of lens are increasingly becoming
the lenses of choice and certainly serve as a most useful problem
solver.
Handling
One of the less talked about benefits of silicone hydrogel
lenses is their ease of handling. Many new young contact lens wearers
have considerable problems associated with the insertion and
removal of their lenses. When this appears likely, I often choose
a silicone hydrogel lens. This is especially the case for teenagers7
who could easily become discouraged because of the awkward aspects
of lens insertion. Parents who are very concerned about their child's
use of lenses are also reassured by the oxygen benefits of the
lenses.
The Aging Eye
There are a group of presbyopes who want to wear contacts for
the first time because of their desire to be able to go to a
social event without wearing glasses. These are usually patients
who have never worn lenses before and are discouraged about their
dependency on bifocal glasses. Many of them have early signs
of corneal edema such as microcysts and small striae. Oxygen
to the cornea becomes an important issue for these patients and
choosing a silicone hydrogel lens reassures the practitioner
about the oxygen needs of the cornea.
The Sleeper
When patients ask to be fitted with
contact lenses, a discussion about sleeping habits should be
part of the history. Many patients nap on commuter trains and
busses, couches during the afternoon or evenings and even during
the opera. These patients deserve the protection of extra oxygen
to reduce their chances of the complications of corneal edema
during lens wear. Practitioners should certainly attempt to fit
all of their "sleepers" in silicone
hydrogel lenses.
AS A PROBLEM SOLVING LENS
Resolving Symptoms of Dryness
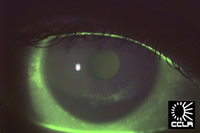 |
Figure 1 - click to enlarge |
The most common complaint of hydrogel lens wearers8
and the most common reason for the discontinuation of soft lens
wear is dryness9;10 . Several studies have shown that symptoms
of dryness, particularly late in the day, are endemic in the
hydrogel lens wearing population8 . As a practitioner who wishes
to keep patients in contact lenses, I spend a good deal of my
clinical hours trying to solve this problem (Figure 1).
The reasons
for the dryness during lens wear are complex. Certainly many
of our patients are of an age when hormone changes, particularly
for women in menopause and those on hormone replacement therapy,
cause ocular surface changes that create symptoms of dryness
even without contact lens wear11 . Hormones affect the tears
in many ways. Testosterone, which is reduced in post menopausal
women and older men, affect the stimulation of the meibomian
glands and the lacrimal glands. Reduced estrogen affects the
mucous membranes of our bodies and is implicated in the drying
of the conjunctiva.
Changes in tear chemistry with age include
reduced tear flow, as measured by the Schirmer test, and complications
associated with poor tear chemistry that lead to increased tear
film evaporation. Tear osmolarity may increase and the secretions
of the meibomian glands may be low or excessive. A mixture of
these changes leads to stimulation of the sensory nerves of the
conjunctiva and cornea, producing the symptoms of discomfort
and dryness. Because of the exposure of the ocular surface to
the elements of the day, these symptoms are increased in the
evening.
Given the sensitivity of the cornea, one would think
that patients would benefit from the protective coverage that
the soft contact lens provides to the cornea. Indeed some patients
do experience real relief when lenses are fitted. For example,
patients who wear soft lenses while cutting onions do not experience
the stinging and excessive tearing that accompanies this task
when lenses are not worn. However, the wearing of these same
lenses causes increased symptoms of discomfort and dryness in
most patients compared to those who do not wear hydrogel lenses.
Apparently the dryness, discomfort sensations differ in origin
or dimension from the stinging sensations and contact lenses
stimulate one and protect from the other. Much more work is required
to determine the factors that affect this most complicated world
of symptoms.
In the meantime practitioners are faced with the
challenge of reducing the symptoms of dryness that threaten continued
contact lens wear. Clinically, we begin with a change of solutions.
Lens wearers who have reduced wear time because of dryness may
benefit from being placed on a non preserved care system such
as Clear Care. By eliminating the preservatives and antibacterial
chemicals that are found in other one step systems, the practitioner
can then decide if the lens itself is the problem. If the symptoms
persist and the lens appears to be the issue then my first choice
for refitting is with a silicone hydrogel lens. Think of the
number of variables that have been changed in this single move:
1.
More oxygen will be available to the cornea. If there was subclinical
oxygen deprivation of the cornea there certainly is no longer.
This fact alone may change the sensory response of the ocular
surface.
In the days of PMMA lens wear and the transition of patients
from the oxygen impermeable material to the oxygen transmission
of the newer rigid lens materials there were many problems. Patients
would return to the clinic after refitting in gas permeables
to say that they did not like the lenses because they were so
much more aware of them in their eyes. This if course was due
to the fact that the cornea had become resensitized and therefore
more symptoms arose. With time the corneal metabolism improved
and the patients adapted to the gas permeable lenses.
My experience
clinically is the same. Some patients have reduced corneal symptomatolgy
associated with their hydrogel lens wear. When first refitted
with silicone hydrogels they are much more aware of the lenses.
With time, however, the cornea reestablishes its healthy normal
metabolism and the lenses feel better.
2. The lens will fit differently.
Silicone hydrogel lenses are stiffer because of the silicone
component and the reduced water content. This makes most patients
more aware of the edges at first. I find that if a carefully
fit the lenses, leaving time for settling and observing the lens
edges, I can determine the best base curve12 and reassure the
patients that this sensation will reduce with wear. In most cases,
on the follow-up visit 2 weeks later, the lens feels comfortable.
3.
There will be less water in the lens and therefore potentially
more water on the eye. When I discuss the concept of refitting
the patient in silicone hydrogel lenses, they always wonder why
I would switch to a lens that is lower in water content. In fact
many of them have experienced my efforts to use higher water
content lenses to improve their comfort. Once I explain that
the lenses leave more of the tear film on the eye instead of
in the lens, they seem satisfied. The proof of the experiment
is always in the wearing and many of my patients are happily
wearing silicone hydrogel lenses with fewer symptoms of dryness.
4. The tear film will interact differently with the contact
lens surface. Many patients who have symptoms of dryness when
wearing their hydrogel lenses have a dry looking lens surface.
Tears that are sludging over the lens must create visual and
physical problems. The tarsal plate has sensory nerve endings
that likely respond to this surface interaction. By dramatically
changing the interaction of the tears and the lens surface, patients
will have a different sensation and hopefully have reduced dryness
and improved comfortable wear time.
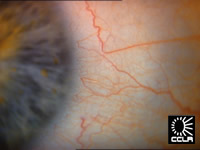
Reducing Redness
Many hydrogel lens wearing patients
present with complaints of red eyes. They are comfortable and
see well but their friends are always asking why their eyes are
so red. This presenting complaint is the most satisfying of all
to address with silicone hydrogel lenses. With almost 100% certainty,
patients experience reduced redness with the wearing of these
lenses13;14 . One of the best clinical ways to demonstrate this
is to use a digital camera to photograph the blood vessels of
the bulbar conjunctiva and limbus at the same time of day on
first visit (Figures 2 and 3, CCLR patient) and 1 to 2 weeks
after wearing silicone hydrogel lenses (Figure 4, same CCLR patient
after 1 week of daily wear with Focus Night & Day). The difference
is clear.
 |
 |
Figure
2 - click to enlarge |
Figure
3 - click to enlarge |
|
Figure
4 - click to enlarge |
Filamentary Keratitis
Patients with severe dry eyes such as those with Sjogren's Syndrome,
can experience extreme discomfort when their corneas form filaments.
These patients must be handled carefully as their autoimmune
disease and dry eyes leave them open to infections and severe
rejection of contact lenses. However, those that can be helped
with the use of lenses often do well with silicone hydrogel lenses
in my practice. Unfortunately many of these patients also have
rheumatoid arthritis and therefore cannot readily handle the
lenses. This can be solved by training family members to remove,
insert and disinfect the lenses. If the patient can tolerate
the lenses the relief is overwhelming and often the cornea will
heal to the point where no lenses need to be worn.
SUMMARY
Silicone hydrogel lenses are an extremely useful tool in fitting
patients and in solving their problems. Clinicians who have not
had occasion to use these lenses should embrace their benefits.
Although not every patient can wear the lenses and some may have
clinical problems directly associated with the lens material,
many patients benefit from the design and oxygen transmissibility.
By using these lenses we can keep more of our patients wearing
contact lenses and prevent some of the complications that have
arisen in the past with more conventional lenses.
Reference List
1. Alvord L, Court J, Davis T, Morgan CF, Schindhelm K, Vogt
J et al. Oxygen permeability of a new type of high Dk soft contact
lens material. Optom.Vis.Sci. 1998; 75 :30-6.
2. Morgan CF, Brennan NA, Alvord L. Comparison of the coulometric
and polarographic measurement of a high-Dk hydrogel. Optometry
and Vision Science 2001; 78 :19-29.
3. Tighe B. In: Sweeney D, ed. Silicone Hydrogels: the rebirth
of continuous wear contact lenses . Oxford: Butterworth-Heinemann,
2000: 1-21.
4. Covey M, Sweeney DF, Terry R, Sankaridurg PR, Holden BA.
Hypoxic effects on the anterior eye of high-Dk soft contact lens
wearers are negligible. Optometry and Vision Science 2001; 78 :95-9.
5. Nilsson SE. Bacterial keratitis and inflammatory corneal
reactions: possible relations to contact lens oxygen transmissibility:
the Harold A. Stein Lectureship 2001. Contact Lens Association
of Ophthalmologists Journal 2002; 28 :62-5.
6. Fonn D, du T, Simpson TL, Vega JA, Situ P, Chalmers RL. Sympathetic
swelling response of the control eye to soft lenses in the other
eye. Investigative Ophthalmology and Visual Science 1999; 40 :3116-21.
7. Soni S, Horner D. Keeping teens healthy in contact lenses. Contact
Lens Spectrum 1995; 10 :20-7.
8. Begley CG, Caffery B, Nichols KK, Chalmers R. Responses of
contact lens wearers to a dry eye survey. Optometry and Vision
Science 2000; 77 :40-6.
9. Pritchard N, Fonn D, Brazeau D. Discontinuation of contact
lens wear: a survey. International Contact Lens Clinic 1999; 26 :157-62.
10. Young G, Veys J, Pritchard N, Coleman S. A multi-centre
study of lapsed contact lens wearers. Ophthalmic and Physiological
Optics 2002; 22 :516-27.
11. Mathers WD, Stovall D, Lane JA, Zimmerman MB, Johnson S.
Menopause and tear function: the influence of prolactin and sex
hormones on human tear production. Cornea 1998; 17 :353-8.
12. Dumbleton KA, Chalmers RL, McNally J, Bayer S, Fonn D. Effect
of lens base curve on subjective comfort and assessment of fit
with silicone hydrogel continuous wear contact lenses. Optom.Vis.Sci. 2002; 79 :633-7.
13. Dumbleton KA, Chalmers RL, Richter DB, Fonn D. Vascular
response to extended wear of hydrogel lenses with high and low
oxygen permeability. Optom.Vis.Sci. 2001; 78 :147-51.
14. Papas EB, Vajdic CM, Austen R, Holden BA. High-oxygen-transmissibility
soft contact lenses do not induce limbal hyperaemia. Current
Eye Research 1997; 16 :942-8.
|



 Barbara
Caffery
Barbara
Caffery