Microbial
keratitis (MK), is a serious but rare complication associated
with contact lens wear, which is considered to be the major predisposing
factor for corneal infection in the United States and Western
Europe.1 When ulceration is severe, the diagnosis of
microbial keratitis is primarily clinical and reasonably straight
forward, and is substantiated largely by microbiological data.
In contact lens practice the practitioner often sees microbial
ulcers at a very early stage, where the diagnosis is entirely
clinical. In these cases, ulceration is usually not severe and
microbiological workup may not be informative. One condition that
is often confused with early stage microbial keratitis is contact
lens-induced peripheral ulcer (CLPU). This article discusses the
various clinical clues that would be helpful in differentiating
the two conditions.
 |
 |
|
Click
to enlarge |
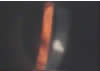
| Figure 1: Pseudomonas keratitis with
contact lens wear. |
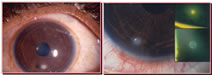
Figure 2: Contact lens induced peripheral
ulcer (CLPU). |
Microbial keratitis (Fig 1) is an infection of the cornea characterized
by excavation of the corneal epithelium, Bowman’s layer,
and stroma with infiltration and necrosis of tissue.2
CLPU (Fig 2) on the other hand is an inflammatory reaction of
the cornea characterized in its active stage by focal excavation
of the epithelium, infiltration, and necrosis of the anterior
stroma. In CLPU, the Bowman’s layer remains intact.3
Clinical Presentation
Patients with MK typically present with significantly more symptoms
than those with CLPU. Pain, redness, photophobia, and lacrimation
are the usual symptoms, even at a very early stage in MK. On the
other hand, patients with CLPU may present asymptomatically or
with mild discomfort. Pain is unusual in a patient with CLPU and
strongly points to MK. Except for lacrimation, discharge is very
unusual in patients with CLPU. Loss of vision is unlikely in either
of the conditions in the early stages of the disease. However,
decrease of vision is almost never a feature of CLPU and strongly
suggests an infectious etiology.
 |
 |
Click
to enlarge |
Click
to enlarge |
| Figure 3: Sectoral congestion limited
to the area of focal infiltrate. |
Figure 4: Pseudoguttate changes on
endothelium in MK. |
Presence of lid edema is a strong pointer to MK and patients
with CLPU usually show no evidence of lid swelling. However, the
absence of lid edema does not rule out the possibility of MK.
In CLPU, bulbar conjunctival injection is restricted typically
to the quadrant where the focal infiltrate is located, whereas
in MK injection is generalized (Fig 3).
Detailed biomicroscopic evaluation will reveal many distinguishing
features between MK and CLPU. The cornea surrounding an infiltrate
is typically clear in CLPU, while in MK some degree of stromal
edema and folds is not uncommon. However, in the early stages
of MK the surrounding cornea may remain clear. Diffuse infiltration
in the anterior layers of the stroma, seen as fine granular collection
of cells, is a typical feature of corneal inflammation. While
infiltration is present in both MK and CLPU, it is localized to
the affected quadrant of the cornea in the latter and is widespread
in the former. Observation of the endothelial surface may reveal
the presence of powdery debris or pseudoguttata in patients with
MK, while it is very unusual to see such changes in CLPU (Fig
4).
 |
Click
to enlarge |
| Figure 5:
Amoeboid shape of focal infiltrate in MK. |
Focal infiltration should be evaluated closely for size, shape,
location, density and overlying epithelial changes. In CLPU, focal
infiltrates are not usually greater than 1.5 mm in diameter but
can be bigger than this in MK. An increase in focal infiltrate
size on follow-up examinations is a strong pointer to MK. In CLPU,
focal infiltrate is round or sometimes slightly oval, whereas
in MK the infiltrate can be of any shape. An irregular shape or
gradual change in the shape of the focal infiltrate, particularly
with an amoeboid extension, is strongly suggestive of MK (Fig
5). In CLPU, the infiltrate is generally located in the periphery
or mid-periphery of the cornea, while in MK it could be closer
to the central portion of the cornea. Often, the focal infiltrate
in CLPU is located in the superior portion of the cornea, which
is normally covered by the upper lid and could be missed on a
cursory examination.
 |
 |
Click
to enlarge |
Click
to enlarge |
| Figure 6a & b: Density of focal
infiltrate: compare the opaque appearance in MK(6a) with the
translucent appearance in CLPU (6b). |
Figure 7 |
In MK, the infiltrate appears solid (opaque), and yellowish or
grayish white, and can appear translucent and lighter in colour
in CLPU (Fig 6a & 6b). In the active stage of both MK and
CLPU, there is a full-thickness epithelial defect overlying the
focal infiltrate. However, patients with MK can present with a
patchy, granular looking infiltrate, without any epithelial defect
and only stipple staining of the overlying epithelium (Fig 7).
Sometimes, seemingly active CLPU may only have punctate epithelial
staining pattern, which may be indicative of a resolving event.
Clinical Course
CLPU is a spontaneously resolving condition, where healing is
facilitated by discontinuation of contact lens wear. Treatment
does not require use of topical antibiotics or steroids. Patients
may occasionally need lubricating eye drops or non-steroidal anti-inflammatory
medication for symptomatic relief. The focal and diffuse infiltrates
resolve over a period of one week, leaving behind a small, faint,
circular scar. On the other hand, treatment of MK requires discontinuation
of contact lens wear and the use of broad-spectrum antibiotics.
It may take longer than a week for MK to resolve and after resolution
there is usually a dense scar. Close follow-up care is critical
in MK in order to resolve the condition at the earliest, while
in CLPU it is necessary in order to avoid misdiagnosis.
Grading
On the basis of the clinical features described, we devised a
scoring system as shown in Table 1. We applied this scoring system
to our database of 44 CLPUs and 6 MKs. The mean scores are shown
in Table 2. Based on these results, we suggest that a score of
7 or less indicates a typical CLPU, up to 10 indicates an atypical
CLPU, and any score of 12 or more is definitive evidence of MK.
Any score beyond 8 should raise a high index of suspicion of MK.
In addition, diagnosis of MK is to be considered if the clinical
picture continues to worsen on discontinuation of contact lens
wear or if the infiltrate increases in size or develops an irregular
shape during follow-up examinations.
Table 1. Scoring
of clinical features |
Parameters |
0 |
1 |
2 |
3 |
Symptoms |
Nil |
Mild |
Moderate |
severe |
Lid edema |
Nil |
- |
Present |
- |
Conjunctival injection |
Nil |
Localized |
Generalized |
- |
Infiltrate Size |
- |
Round |
- |
Irregular |
| Shape |
- |
< 1.0 mm |
> 1.0 mm |
> 2.0 mm |
Epithelial defect |
Nil |
Yes |
- |
- |
Surrounding cornea |
Clear |
Edema |
Edema / Descemet's folds |
- |
Endothelial debris |
Nil |
Present |
- |
- |
Hypopyon |
Nil |
- |
Yes |
- |
Effect of discontinuation from lens
wear |
Resolving |
Status quo |
Increase in signs |
Increase in signs and symptoms |
Table 2. Scoring
of typical CLPU, Atypical CLPU and MK |
Parameters |
Mean (range)
|
|
Typical CLPU |
Atypical CLPU |
MK |
|
(n
= 36) |
(n
= 80 |
(n
= 6) |
Symptom |
1.60 (1-2) |
2.75 (2-3) |
3 (3) |
Lid edema |
0 (0) |
0.75 (0-2) |
1 (0-2) |
Conjunctival injection |
1.75 (1-2) |
2 |
2 |
Infiltrate - Shape |
1 |
1 |
2.66 (1-3) |
Infiltrate - Size |
1.08 (1-2) |
1.13 (1-2) |
2.3 (1-3) |
Epithelial defect |
0.77 (0-1) |
0.75 (0-1) |
1 |
Surrounding cornea |
0 (0) |
0 (0) |
0 (0) |
Endothelial debris |
0 (0) |
0.25 (0-1) |
0.83 (0-1) |
Hypopyon |
0 (0) |
0 (0) |
0 (0) |
Effect of discontinuation |
0.05 (0-2) |
0.75 (0-2) |
1.5 (1-3) |
Total score |
6.27 (3-7) |
9.25 (9-10) |
14.16 (12-17) |
Role of Microbiology
Although this article emphasizes the clinical aspects of differentiation
between MK and CLPU, it is important to identify the role of microbiological
investigations under some circumstances. We did not obtain any
useful information from microbiological workup, if the focal infiltrate
measured 1.0 mm or less. If the lesion is larger (>1.5 mm)
or not responding to the conventional treatment, it is imperative
that proper microbiological workup be done.
Conclusion
Differentiating MK and CLPU is important in contact lens practice
in order to avoid unnecessary treatment and prevent possible complications.
These two conditions can mimic each other causing a diagnostic
dilemma. While it is possible to differentiate them clinically,
a high index of suspicion needs to be exercised to avoid misdiagnosing
MK. While practitioners with experience can have their own diagnostic
criteria, those who have not seen many of these events can use
the provided information and the scoring system to facilitate
in the diagnosis. However, when in doubt it is better to seek
a second opinion or treat the condition as MK.
Murali K Aasuri, M.D
Nagaraju Venkata, B.Optom
Vinod M Kumar, DOT
Prof. Brien Holden Eye Research Centre,
L V Prasad Eye Institute,
Hyderabad, India.
|



 Murali
K Aasuri - MD
Murali
K Aasuri - MD