With the invention of silicone hydrogel (SH) contact lenses most hypoxia related complications are reduced and when comparing ocular health between SH contact lens wearers and non lens wearers, only the level of conjunctival staining in SH lens wearers was greater. [1]
One of the most oxygen sensitive parts of the eye is the corneal endothelium which consists of a single cell layer with a thickness of approximately 5microns. [2] Reduced oxygen supply causes different short and/or long term responses and has been observed with all types of low DK contact lenses (DK=oxygen permeability). [3, 4] But what can be expected, if habitual hydrogel lens wearers are refitted with SH lenses?
A typical short term response to contact lens wear is the occurrence of endothelial blebs. These oedematous cells (blebs) or ‘dark spots’ in the endothelial mosaic occur as a result of increased carbonic acid and lactic acid levels fairly soon after insertion of a low DK lens. [3, 5] Brennan and coworkers reported on a contralateral study in which they determined the number of blebs after 20 minutes of lens wear. Under closed eye conditions, they found an average of 7.4 blebs per 100 cells in the eye with a low DK lens (polymacon) and an average of 1.9 in the eye wearing a high DK SH lens (senofilcon A). [6] They further investigated different SH materials worn under open eye conditions and reported on less than 1 bleb per 100 cells for all SH materials investigated (galyfilcon A, senofilcon A and lotrafilcon A). A similar relation between the oxygen permeability of the lens material and the formation of blebs have been shown by Hamano et al, [7] who further reported on higher bleb rates in Asian eyes compared to Non-Asian eyes under the same lens wear conditions. [7] Endothelial bleb formations are described as a short term response and typically disappears approximately 10 minutes after lens removal. [6]
Long term morphological changes of the endothelium increase with age, and are often seen with adapted low DK lens wearers (Figure 1a+b). [4] The most typical conditions are described as follows:
Polymegathism – Variation in cell size increases, typically expressed as Coefficient of Variation (COV)
Pleomorphism – Variation in cell shape increases, typically expressed as percentage of hexagonal cells.
Cell Density - Number of cells for a given area decreases, typically expressed as cells/mm2
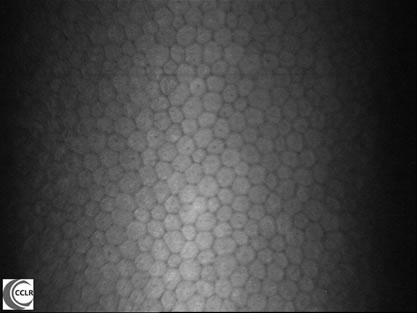
Figure 1a
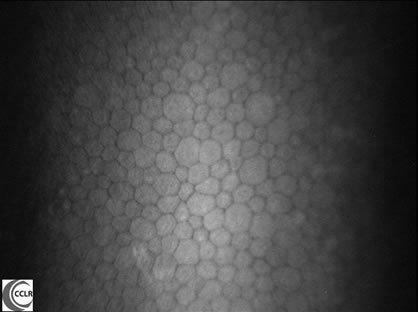
Figure 1b
Figure 1 a+b: Confocal images of the corneal endothelium with a) normal structure and b) moderate levels of polymegathism and pleomorphism (Nidek ConfoScan3, 500x magnification - Simone Schneider, Centre for Contact Lens Research)
Whether or not a refit with SH lenses can reduce these changes in the endothelial structure has been investigated by Doughty and coworkers. [8] In this study low DK hydrogel lens wearers with a history of approximately 5 years of successful daily lens wear were refitted with SH lenses (lotrafilcon A) for continuous wear over 30 days and nights. Endothelial conditions were evaluated at study entry and after 6 months of SH wear. A small decrease in polymegathism was found (COV decreased from 30.2% to 29.1%) and a small reduction in pleomorphism showed a slightly higher content of hexagonal cells (58.3% to 60.1%). However they also reported on a decrease/redistribution in central cell density (from 2821 to 2774 cells/mm2); nevertheless none of these trends reached statistical significance. [8]
A similar study was conducted by Aakre and colleagues over the same study period of six months. [9] Participants in this study had a lens wear history of approximately 10 years and were either refitted with daily disposable hydrogel lenses (nefilcon A, etafilcon A or hilafilcon A) or high DK SH lenses (lotrafilcon A or balafilcon A). They found a minor decrease in pleomorphism for the SH group but overall no significant difference was detected in the endothelial structure comparing the SH group with the daily disposable lens wearers, which was similar to a study conducted by Brennan. [6]
Edmonds and colleagues are currently the only researchers that presented results from a pilot study that showed a small but significant decrease in polymegathism after refitting adapted low DK lens wearers with lotrafilcon A SH lenses. [10]
Corneal endothelial cells are very unique as they do not divide or replicate and invasive morphological changes cannot recover as seen with corneal epithelial cells. Changes in the endothelium due to low DK lens wear are sometimes accompanied by corneal swelling and a recent study by Morgan [11] did confirm that all low DK hydrogel materials induced some level of swelling, but none of the five investigated SH materials caused a change in corneal thickness under open eye conditions.
Studies to-date suggest that fitting adapted hydrogel lens wearers with SH lenses reduces short term endothelial responses; however the recovery from long term structural changes has not been conclusively established. The endothelial structure in long term SH lens wearers on the other hand appears to be similar when compared to non lens wearers even after 9 months of continuous lens wear of lotrafilcon A. [1] The message is clear: We can prevent the occurrence of long and short term endothelial responses by choosing SH over conventional hydrogel lenses in new lens wearers.
- Covey M, Sweeney DF, Terry R, Sankaridurg PR, Holden BA. Hypoxic effects on the anterior eye of high-Dk soft contact lens wearers are negligible. Optom Vis Sci 2001;78(2):95-9.
- Remington LA. Cornea and sclera. Clinical anatomy of the visual system. St. Louis, Mo.: Elsevier-Butterworth Heinemann; 2005. p 9-33.
- Efron N. Contact lens-induced changes in the anterior eye as observed in vivo with the confocal microscope. Prog Retin Eye Res 2007;26(4):398-436.
- Lee JS, Park WS, Lee SH, Oum BS, Cho BM. A comparative study of corneal endothelial changes induced by different durations of soft contact lens wear. Graefes Arch Clin Exp Ophthalmol 2001;239(1):1-4.
- Holden BA, Williams L, Zantos SG. The etiology of transient endothelial changes in the human cornea. Invest Ophthalmol Vis Sci 1985;26(10):1354-9.
- Brennan NA, Coles ML, Connor HR, McIlroy RG, Gavras S, Moody KJ, Henderson T. Short-term corneal endothelial response to wear of silicone-hydrogel contact lenses in East Asian eyes. Eye Contact Lens 2008;34(6):317-21.
- Hamano H, Jacob JT, Senft CJ, Hamano T, Mitsunaga S, Kotani S, Kaufman HE. Differences in contact lens-induced responses in the corneas of Asian and non-Asian subjects. Clao J 2002;28(2):101-4.
- Doughty MJ, Aakre BM, Ystenaes AE, Svarverud E. Short-term adaptation of the human corneal endothelium to continuous wear of silicone hydrogel (lotrafilcon A) contact lenses after daily hydrogel lens wear. Optom Vis Sci 2005;82(6):473-80.
- Aakre BM, Ystenaes AE, Doughty MJ, Austrheim O, Westerfjell B, Lie MT. A 6-month follow-up of successful refits from daily disposable soft contact lenses to continuous wear of high-Dk silicone-hydrogel lenses. Ophthalmic Physiol Opt 2004;24(2):130-41.
- Edmonds C, Bullimore MA, Sheng H, Chalmers R. Endothelial morphology 1 year after refitting hydrogel lens wearers with lotrafilcon A silicone hydrogel lenses. Optom Vis Sci (E-Abstract 045095); 2004.
- Morgan PB, Brennan NA, Maldonado-Codina C, Quhill W, Rashid K, Efron N. Central and peripheral oxygen transmissibility thresholds to avoid corneal swelling during open eye soft contact lens wear. J Biomed Mater Res B Appl Biomater 2010;92(2):361-5.
|



 Doerte Luensmann, PhD
Doerte Luensmann, PhD